Introduction
The appropriate use of a laryngoscope demands the patient to be in a typical posture with their mouth open, chin raised, and neck tilted back. However, certain patients need restrictions in the movement of their cervical spine that may require the head to be in a neutral position [1]. Therefore, using a semi-rigid neck collar can maintain a neutral head and neck position, but this allows very little movement of the neck and limits sufficient mouth opening. Unfortunately, this can deteriorate the environment for tracheal intubation and may lead to hypoxia or tissue damage [2ŌĆō4]. Although advances in videolaryngoscopes have made tracheal intubation easier for patients with restricted cervical spine movement, patients with semi-rigid neck collars still need more adequate and established intubation techniques.
In the conventional Macintosh blade technique for orotracheal intubation, a blade tip is placed on the vallecula and lifts the glottis. Another recommended technique of handling a blade is inserting the blade under the epiglottis in case of a damaged or protruding tooth or if the patient has a soft epiglottis [5ŌĆō7]. A cadaver study investigated inserting a laryngoscope with manual in-line stabilization for cervical spine fixation. They found that a straight blade designed to directly lift the glottis, similar to placing the blade tip under the epiglottis, could improve the intubation environment more than a curved blade [8].
Videolaryngoscopes have lenses mounted at the end of the blade and the tip as well as fiberscopes. Partly resembling the technique used in the maneuver of the flexible fiberoptic bronchoscope, gliding a blade of the videolaryngoscope under the epiglottis to expose vocal cords can achieve a better glottic view. However, the best technique for handling the blade of videolaryngoscopes in patients with a semi-rigid neck collar has not yet been definitely established.
Therefore, we aimed to compare the overall intubation environment, including the glottic view, obtained with a videolaryngoscope using the technique of gliding a blade under the epiglottis and the conventional Macintosh blade technique of placing a blade tip on the vallecula in patients wearing a semi-rigid neck collar undergoing cervical spine surgery.
Materials and Methods
Participant enrolment and assignment
This prospective randomized parallel study was conducted at Gangnam Severance Hospital, Yonsei University Health System, Seoul, Republic of Korea, in accordance with the Declaration of Helsinki 2013. The study protocol was approved by the Institutional Review Board and Hospital Research Ethics Committee of Gangnam Severance Hospital, Yonsei University Health System (IRB No. 3-2020-0318) on September 1, 2020, and registered at ClinicalTrials.gov (NCT04578119) on October 19, 2020. Written informed consent was obtained from all the participants. Patients aged Ōēź 20 years with an American Society of Anesthesiologists physical status IŌĆōIII scheduled for elective cervical spine surgery in the neurosurgery department at our institution between October 2020 and August 2021 were assessed for eligibility. Patients requiring rapid sequence induction or planned awake intubation, those with symptomatic asthma or reactive airway disease requiring daily pharmacological treatment, and those with the inability or unwillingness to provide informed consent were excluded.
On the day of the surgery, the patients were randomly allocated to undergo orotracheal intubation either by placing the blade tip on the vallecula (conventional group) or by gliding it under the epiglottis (gliding group). The allocation was performed in a 1 : 1 ratio based on a computer-generated sequence using permuted block randomization with a block size of four. Copies of the random sequence were kept in sealed opaque envelopes that were opened by only two attending anesthesiologists immediately before anesthesia induction, following which intubation was performed in the assigned groups.
Preparation and anesthesia
A researcher, blinded to the group assignment, performed an airway assessment in the preoperative holding area. The MallampatiŌĆÖs classification score, thyromental distance, inter-incisor distance (before and after semi-rigid neck collar placement), and neck circumference were measured. The condition of the teeth (no teeth, missing, mobile, or broken teeth, and partial or complete dentures), limited range of the cervical spine movement (extension, flexion, and instability), and inability to protrude the lower jaw (< 1 cm) were also checked. Subsequently, the Stifneck Select┬« Collar (Laerdal Medical Corp., Norway)ŌĆöa semi-rigid neck collarŌĆöwas worn by all patients. Upon arrival at the operating room, electrocardiography, pulse oximetry, non-invasive blood pressure measurement, and bispectral index monitoring were performed. After the patients were preoxygenated with 100% oxygen for 3 min, remifentanil (0.2ŌĆō0.4 ╬╝g/kg/min), propofol (1% 1.5ŌĆō2.0 mg/kg), and rocuronium (0.8ŌĆō1.0 mg/kg) (degree of muscle relaxation appropriate for tracheal intubation: train-of-four, 0/4) were administered to induce anesthesia.
Intubation technique
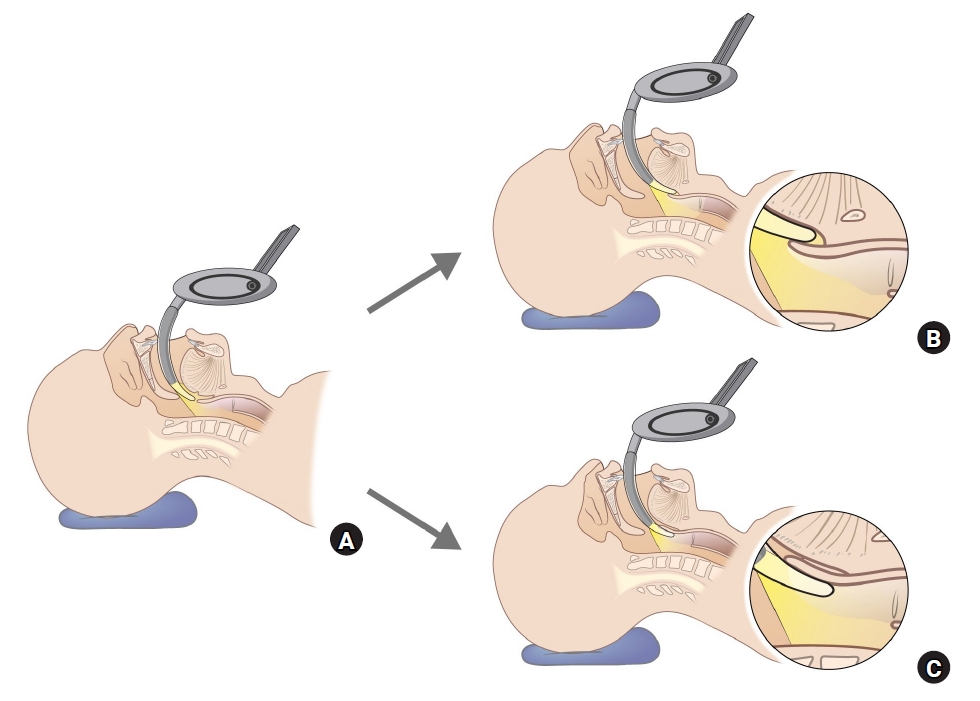
Orotracheal intubation was performed by two attending anesthesiologists with at least 10 years of experience and who had used the McGrathTM videolaryngoscope (Medtronic, UK) 100 times or more. They had prior experience with the gliding technique using the McGrathTM videolaryngoscope, each having managed at least 50 cases. Cuffed Mallinckrodt Hi-Contour Tracheal TubesTM (Covidien, USA; 7.0 mm for females, 8.0 mm for males) were used, and malleable stylets (Satin-Slip┬«; Mallinckrodt Inc., USA) were mounted on the tubes. The stylets were prepared with the distal end angulated to a ŌĆśhockey stickŌĆÖ shape (Hockey-Stylet) that consisted of a 100┬░ angle created 8 cm from the distal tip of the cuffed tracheal tube, as this was reported to be the best shape in a previous study [9]. We inserted a blade of McGrathTM videolaryngoscope into the patientŌĆÖs mouth in the midline, and the tip of the blade was then guided around the base of the tongue. After the blade approached the epiglottis, in the conventional group, the blade tip was placed on the vallecula and tilted to lift the epiglottis anteriorly, similar to the conventional Macintosh blade technique. In the gliding group, a blade was introduced from the epiglottis tip to the posterior wall of the epiglottis that partly resembled the maneuver of a flexible fiberoptic bronchoscope without aligning the axis by moving the blade anteriorly. As the vocal cords became visible, the blade was glided in a little more (Fig. 1).
Outcomes assessment
The primary outcome was the percentage of glottic opening (POGO) score [10]; two independent investigators, who were not involved in the real intubation procedure, evaluated the POGO scores. An image of the glottic views was captured on the monitor display when an optimal view of the glottis was obtained, and intubation was conducted. Successful tracheal intubation was confirmed by auscultation of both sides of the chest and end-tidal carbon dioxide graphs on the ventilator monitor. More than two intubation attempts were considered failure of intervention in our study protocol; such cases were dropped out from the study. The time taken to obtain an optimal visual condition (optimal glottic view)ŌĆöin other words, the time until the glottic view with the best POGO score was securedŌĆöwas evaluated as that shown at the final (successful) attempt; the time taken to confirm successful tracheal intubation (duration of intubation) was recorded as the total time from the first attempt to the final successful intubation. Additional aid for making good processing of intubation that included manipulation of backward, upward, and rightward pressure (BURP) was also assessed. Moreover, an independent researcher asked the researcher who performed the intubation whether there was an upward lifting force of the hand while handling the blade and recorded the answer. The Intubation Difficulty Scale (IDS) [11] score was determined based on documented data. Following tracheal intubation, the CormackŌĆōLehane (CL) grade [12] and the ease and satisfaction in performing intubation were recorded on a scale of 1ŌĆō5 (1, worst; 5, best), respectively by two attending anesthesiologists. Injury to the patientsŌĆÖ lips, mucosa, or teeth during the intubation process was checked, and the hemodynamic parameters were also monitored. Following extubation, all complications associated with intubation, including hypoxic events (reduction of oxygen saturation to < 90%), lip injury, mucosal bleeding, tooth damage, sore throat, difficulty in swallowing, and voice changes, were assessed in the post-anesthetic recovery room and the ward.
Statistical analysis
In a previous study [13], intubation with the McGrathTM videolaryngoscope showed average POGO scores and standard deviations (SD) of 82 and 23, respectively. We assumed that the POGO score differs by an average of Ōēź 10 points when using the gliding technique compared to the conventional Macintosh blade technique. Considering this, with a power of 80%, significance level of 5%, and drop-out rate of 5%, we calculated the sample size to be 178 participants (89 per group). The KolmogorovŌĆōSmirnov test was used to determine the distributions of all continuous variables. StudentŌĆÖs t-test was performed for normally distributed data, while the MannŌĆōWhitney U test was used for data that were not normally distributed. Chi-square or FisherŌĆÖs exact tests were used to analyze the frequency variables. The inter-rater reproducibility of the POGO measurements was also assessed in all datasets by calculating the intraclass correlation coefficient and coefficient of variation. All data were analyzed using IBM SPSS Statistics for Windows Version 25.0 software (IBM Corp., USA). Differences were considered significant at P < 0.05.
Results
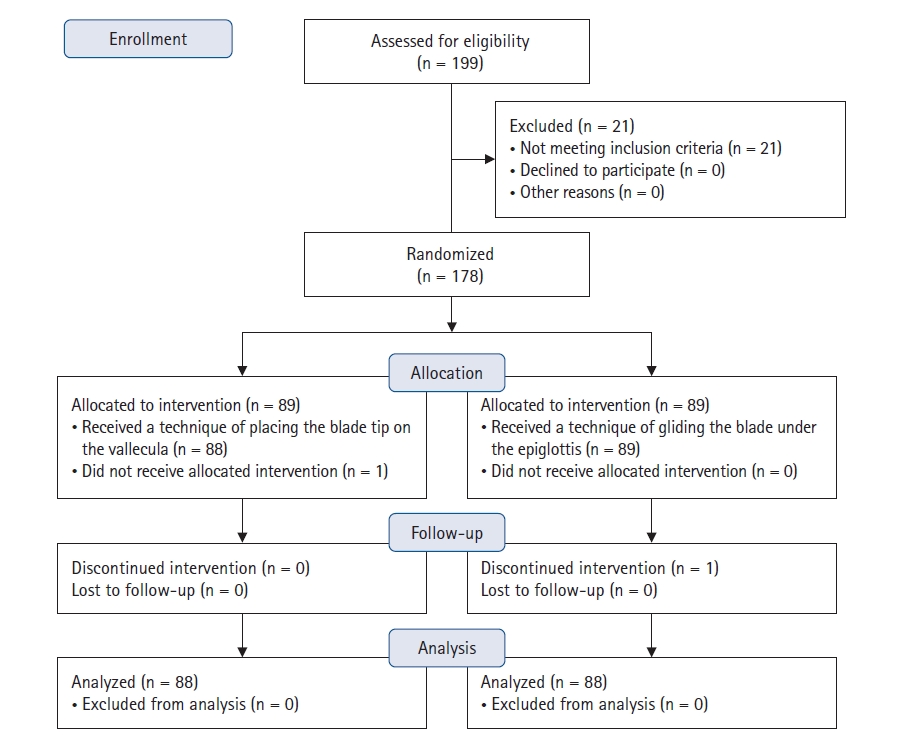
Of the 199 patients assessed for eligibility, 21 were excluded. Therefore, 178 patients were randomized to either the conventional or gliding group; two dropped out, and 88 patients in each group were ultimately analyzed (Fig. 2). There were no differences in patient- and surgery-related characteristics, as well as pre-anesthesia airway assessments between the groups (Table 1).
Table 2 describes the comparison of the POGO scores. The average POGO scores were significantly higher in the gliding group compared with those in the conventional group (88.9 ┬▒ 14.7 vs. 63.8 ┬▒ 27.4, P < 0.001). The inter-rater reproducibility for estimating the POGO score was excellent, with an intraclass correlation coefficient of 0.93 (95% CI [0.90, 0.94]) and a coefficient of variation of 9.2% (within-subject SD 7.0%).
Table 2 also presents parameters related to the intubation environments. The time to obtain an optimal view for intubation and the duration of intubation were significantly shorter in the gliding group than in the conventional group (19.0 [6.9] vs. 27.5 [15.6] s and 45.8 [8.2] vs. 55.8 [15.5] s, respectively; P < 0.001). The CL grade was significantly different between the groups (P < 0.001), and more patients required lifting force and BURP manipulation in the conventional group than in the gliding group (59 [67%] vs. 23 [26.1%] patients and 23 [26.1%] vs. 6 [6.8%] patients, respectively; P < 0.001). In addition, IDS scores were significantly different between the groups (P < 0.001), and both the ease and satisfaction of the anesthesiologists in terms of performing intubation were superior in the gliding group than in the conventional group (P < 0.001). Vital signs, such as blood pressure, heart rate, and peripheral saturation, were comparable between the groups at baseline and before and after intubation (Supplementary Table 1).
Table 3 shows the profile of intubation-related complications. These were not significantly different between the two groups, and all patients were discharged without residual complications.
Discussion
In the present study, a superior laryngoscopic view and more favorable intubation environment were observed with the gliding blade technique than with the conventional Macintosh blade technique in patients undergoing cervical surgery where the cervical movement and mouth opening are restricted with a semi-rigid neck collar. The primary outcome was the laparoscopic glottic view measured using POGO scores when performing intubation with a McGrathTM videolaryngoscope in patients undergoing cervical spine surgery with the need for cervical immobilization. Usually, the quality of the glottic view can be graded using the CL grading system; however, it has several problems, including grade ambiguity between grades 1 and 2 [12,14], and the CL description of the view is not quantitative. For this reason, alternate systems of description, such as the POGO scale [15], have been described that require the viewer to estimate a numerical score; these have the advantage of better inter-rater reliability [15,16]. The POGO score also appears superior to the CL scale in comparing devicesŌĆösuch as videolaryngoscopesŌĆöthat always provide grade 1 on the CL scale [17]. The findings of our study regarding the POGO score, CL grade, and IDS score indicated that the gliding technique is better than the conventional Macintosh blade technique for intubation using a videolaryngoscope.
Cervical immobilization significantly deteriorates ideal intubation conditions in emergency rooms or operating theaters [1]. It may preclude adequate alignment of the oral, pharyngeal, and tracheal axes, thus jeopardizing the visualization of the glottis when using a direct laryngoscopy [3]. Additionally, wearing a neck collar has been associated with a decreased ability to open the mouth [3,4] that limits the direct view that can be captured with a laryngoscope and consequently reduces the success rate of tracheal intubation [18]. In such situations, intubation using a flexible fiberoptic bronchoscope is a reliable approach to acquire a high success rate of tracheal intubation and minimize cervical spine movement. However, the loss of pharyngeal muscle tone under general anesthesia narrows the oropharyngeal space necessary for the flexible fiberoptic bronchoscope to pass through and makes it difficult to maintain the flexible fiberoptic bronchoscope in the midline while advancing its tip into the pharynx and the laryngeal inlet [19ŌĆō21]. Moreover, a well-trained and experienced anesthetist is required for flexible fiberoptic bronchoscope-guided intubation. Hence, several studies have attempted using videolaryngoscopes for intubation of patients requiring cervical immobilization [22ŌĆō24].
Macintosh blade technique is generally used for intubation using a videolaryngoscope as well as a direct laryngoscope. However, since videolaryngoscopes use the indirect glottic view of the camera close to the glottis, it is considered more appropriate to have the blade glide gently under the epiglottis to expose the glottis [25]. As the camera lens of a videolaryngoscope is in the pharynx in any case, the alignment of the airway axes is not important for the maneuver of a flexible fiberoptic bronchoscope. It can easily enter the posterior aspect of the epiglottis; therefore, it is less affected by the anatomy of the larynx. Nevertheless, a good laryngeal view does not always translate to easy intubation [26,27]. In particular, proximal placement of a blade of the videolaryngoscope results in poor glottis visualization (higher CL grades and lower POGO scores). This may be pointed out as a noticeable weakness of using videolaryngoscopy. Therefore, the clinical significance of our results is inevitably substantial because the technique of gliding a blade under the epiglottis similar to that used during the maneuver of a flexible fiberoptic bronchoscope provided an optimal glottic view and increased ease of orotracheal intubation.
Failure to perform adequate immobilization of the cervical spine during orotracheal intubation in patients with cervical spine instability or at risk of spinal cord injury can potentially lead to devastating neurological outcomes. A recent case report described a patient with ankylosing spondylitis who experienced substantial cervical spine injury following videolaryngoscopy intubation [28]. International guidelines recommend manual or mechanical cervical immobilization for trauma patients who require tracheal intubation because of the possibility of radiological or clinical cervical cord injury [29]. Although both manual in-line stabilization and cervical collar are preferred techniques to maintain cervical spine immobility during tracheal intubation, the latter has been shown to limit cervical spine displacements more during orotracheal intubation [8,30]. Accordingly, several studies have simulated difficult intubation by applying a cervical collar to a mannequin; only a few studies have conducted the same investigation in a real clinical field [31ŌĆō35]. We applied a semi-rigid neck collar to patients who actually needed cervical immobilization during intubation for safety and did not intentionally simulate a difficult airway situation.
There were a few limitations in our study. First, we could not blind the intubating anesthetists to the randomization of the videolaryngoscope. However, the POGO scores were obtained by two independent (blinded) investigators who were not involved in intubation, and the other data were also well defined and objective. Moreover, inter-rater producibility between the two investigators who assessed the POGO scores was reliable. Second, this study was conducted by an experienced anesthetist, and the results may vary when applied in other clinical situations. Moreover, the gliding intubation technique presented in our study may have potential risks that have not yet been fully proven; hence, caution is necessary when applying it in clinical practice. However, the McGrathTM videolaryngoscope was used according to the guidelines as much as possible, and the difference between the two groups was adequately clear. In addition, the strength of our findings was that our results were obtained in a real clinical setting. While most previous studies were conducted using mannequins and showed results of airway assessment in a simulated difficult airway situation, our study has great clinical significance as it sought a better orotracheal intubation method by applying it to actual patients.
In conclusion, the technique of gliding a blade under the epiglottis improved the intubation environment compared with the conventional Macintosh blade technique when using the videolaryngoscope in patients with a semi-rigid neck collar. Moreover, tracheal intubation was performed in a shorter duration with more ease and satisfaction for the anesthetists. We expect that intubation with a McGrathTM videolaryngoscope using the gliding blade technique will be greatly helpful in an emergency setting for patients with cervical spine instability who require a semi-rigid neck collar.