Analgesic effects and distribution of cutaneous sensory blockade of quadratus lumborum block type 2 and posterior transversus abdominis plane block: an observational comparative study
Article information

Abstract
Background
The posterior transversus abdominis plane block (TAPB) and quadratus lumborum block (QLB) were developed for postoperative pain control after lower abdominal surgery. However, there is little data regarding their effects. Their analgesic effects and the distribution of the cutaneous sensory blockade were observed in patients undergoing laparoscopic gynecologic surgery.
Methods
After an induction of general anesthesia, patients alternately received bilateral ultrasound-guided QLB type 2 (QLB2) or posterior TAPB using 20 ml of 0.375% levobupivacaine on each side. The measurements included visual analogue pain scores (VAS), cutaneous sensory blockade in each dermatome, demands for postoperative analgesics, and complications for up to 48 h after the block. Our primary endpoint was VAS at 24 h after the block.
Results
Forty patients completed the study. The VAS at rest was significantly lower after QLB2 than that after TAPB at 48 h, but not at 24 h. Neither group differed in VAS when coughing at any point in time. Postoperative demands for fentanyl and other analgesics also did not differ for either block. The majority of injections produced a cutaneous sensory blockade in the T11 and T12 dermatomes in both groups. The median number of dermatomes blocked was limited to three dermatomes after either block. No severe complication related to either block was observed.
Conclusions
The analgesic effects of QLB2 and posterior TAPB did not differ in patients undergoing laparoscopic gynecologic surgery. The cutaneous sensory blockade produced was limited to three dermatomal levels in the majority of patients. However, these findings need to be confirmed through a larger comparative study.
Introduction
Laparoscopic gynecologic surgery is thought to be minimally invasive. Nevertheless, patients need sufficient postoperative analgesia through the use of opioids [1]. However, opioids cause complications such as respiratory depression, postoperative nausea, and vomiting. Multimodal analgesia including abdominal wall blocks can reduce opioid consumption and provide better analgesic effects [2,3]. Since the first description of an ultrasound-guided (US-guided) technique [4], the transversus abdominis plane block (TAPB) has become popular, and several techniques [5,6] have been developed. Among them, posterior TAPB, which is conducted by injecting local anesthetic close to the lumbar triangle of the Petit, may result in postoperative analgesia that is superior to and longer than lateral TAPB with the injection made more anteriorly [7,8]. The quadratus lumborum block (QLB) was introduced more recently as a technique for injecting a local anesthetic solution more posteriorly and along the quadratus lumborum muscle [9]. Among the approaches that have been developed for QLB, the posterior approach to QLB called QLB type 2 (QLB2) is thought to produce effective and long-lasting analgesia after abdominal surgery [9–11].
A previous retrospective study on children [12] showed that posterior TAPB produces a cutaneous sensory blockade at T7–T12. However, no known study has examined whether posterior TAPB and QLB2 are different in terms of sensory blocks and postoperative analgesia. The distribution of a cutaneous sensory blockade and the analgesic effects of these techniques remain to be explored in detail. Therefore, in this prospective study, we observed and compared the analgesic effects and the distribution of a cutaneous sensory blockade in patients undergoing laparoscopic gynecologic surgery.
Materials and Methods
The study protocol was approved by the Shimane University Hospital ethical committee (study no. 2140) and was registered in the University Hospital Medical Information Network Clinical Trials Registry (UMIN000021662). The study was planned to be conducted between March 29, 2016 and September 30, 2017. We obtained written informed consent from patients 20–70 years in age with the American Society of Anesthesiologists physical status I and II, who were scheduled for laparoscopic gynecologic surgery. Patients with contraindications to the peripheral nerve blocks, a history of diabetes mellitus, or neurologic disease were excluded. We alternately assigned patients to either the QLB group (receiving QLB2) or TAPB group (receiving posterior TAPB).
In the operating room, the patient’s electrocardiogram, heart rate, and oxygen saturation were continuously monitored and their non-invasive blood pressure was recorded every 5 min. General anesthesia was induced using propofol and fentanyl 2–4 µg/kg. Rocuronium was used to facilitate tracheal intubation. After tracheal intubation, patients received either QLB2 or posterior TAPB accordingly. The blocks were performed with the patient in either a supine or slightly wedged position. The anesthetist performing each block could use either a 6–13 MHz linear (S-nerve, Fujifilm SonoSite, Inc., Japan) or 2–5 MHz convex (S-nerve, Fujifilm SonoSite, Inc., Japan) transducer to apply the block. The skin was prepared using chlorhexidine, and the ultrasound transducer was covered using a sterile plastic cover and gel. The transducer was initially positioned at the lateral abdomen between the iliac crest and the costal margin. The ultrasound view was adjusted to show the external oblique, internal oblique, and transversus abdominis muscles. The quadratus lumborum muscle was observed posterior to the transversus abdominis muscle, as the transducer was moved more posteriorly. A 21-gauge block needle (Sonoplex 100 mm; PAJUNK, USA) was inserted from the lateral abdomen and advanced in an anterolateral to posteromedial direction in plane with the ultrasound beam (Fig. 1). For the TAPB group, the needle was advanced to reach between the internal oblique muscle and near the posterior end of the transversus abdominis muscle. For the QLB group, the needle was inserted similarly to that used for TAPB but advanced to reach the posterolateral area of the quadratus lumborum muscle and the lumbar interfascial triangle (LIFT) between the quadratus lumborum, erector spinae, and latissimus dorsi muscles (Video 1). Before surgery, each group received bilateral blocks with 20 ml of 0.375% levobupivacaine for each side. All blocks were either performed or directly supervised by an anesthetist (S.S.) with extensive experience in peripheral nerve blocks. The same gynecological team conducted all surgical procedures. Laparoscopic surgery was conducted using a 12 mm port at the umbilicus and the right lower abdominal part, and using a 5 mm port at five fingerbreadths below the umbilicus and the left lower abdominal part. Intraoperatively, general anesthesia was maintained using propofol titrated to maintain a bispectral index of 40–60 and remifentanil at 0.1 µg/kg/min. When the heart rate and/or blood pressure increased by more than 20% from the baseline, 1 µg/kg of fentanyl was added intravenously to maintain hemodynamic stability. Rocuronium was administered intermittently during the operation. After surgery, sugammadex sodium was administered to reverse the muscle relaxation, and the trachea was extubated when the patients were fully awake and breathing adequately. All patients received an intravenous basal infusion of fentanyl at 20 µg/h starting at the end of surgery, and an on-demand bolus of 10 µg with a 10-min lockout time for patient-controlled analgesia (PCA). The continuous infusion of fentanyl was discontinued when the patient reported severe postoperative nausea or vomiting. Patients in the ward received loxoprofen sodium hydrate 3 times a day as well as other analgesics including acetaminophen and diclofenac sodium upon request.
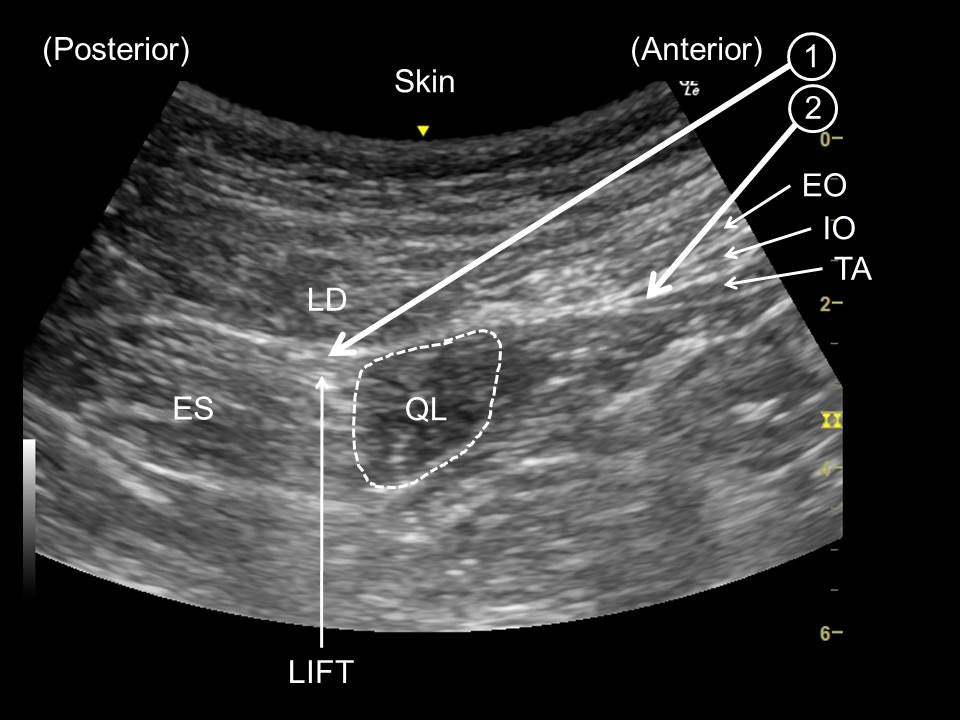
Ultrasound image showing needle approach. ① Quadratus lumborum block type 2. ② Posterior transversus abdominis plane block. EO: external oblique muscle, IO: internal oblique muscle, TA: transversus abdominis muscle, LD: latissimus dorsi muscle, QL: quadratus lumborum muscle, ES: Erector spinae muscle, LIFT: lumbar interfascial triangle.
The patients were blinded to their group assignment. Anesthetists who were blinded to the group allocation conducted the measurements postoperatively at 6, 12, 24 and 48 h after the blocks. The measurements included the following parameters: visual analogue pain score (VAS) (0 mm, no pain; 100 mm, worst pain imaginable) at rest and while coughing, postoperative cumulative fentanyl consumption and the use of other analgesics, a cutaneous sensory blockade at each dermatome, postoperative nausea or vomiting, and complications related to the blocks. A cutaneous sensory blockade was assessed bilaterally on the anterior axillary line using ice cubes and a 22-gauge slightly dulled needle for loss of cold and pin-prick sensations, respectively.
Statistical analysis
We hypothesized that the VAS at rest 24 h after the blocks, which was the primary outcome of this study, was lower after QLB2 than after posterior TAPB. The sample number was determined based on our preliminary data showing a mean VAS of 16 mm and a SD of 14 mm at rest 24 h after receiving the posterior TAPB, and a minimum change in the clinical significance of the VAS, which was previously shown to be 13 mm [13]. The sample size calculation conducted using G*Power (version 3.1, Cognitive and Industrial Psychology, Heinrich-Heine-Universtaet, Germany), under the assumption of α = 0.05 and β = 0.2 (80% power), showed that 20 samples were required for each group. Our institutional ethical committee did not give permission for a randomized controlled trial based on the fact that no prior results comparing the two techniques were available at the time. Therefore, we alternately allocated patients to either the QLB group to receive QLB2 or to the TAPB group to receive posterior TAPB. The study was continued until we were able to collect data from at least 20 patients for each group.
Continuous data were analyzed through a Kolmogorov–Smirnov test to determine the normality of the data distribution. A two-tailed Student’s t-test was applied for the parametric statistics, and the result was expressed as mean ± SD. A Mann-Whitney U-test was applied for non-parametric statistics and the result was expressed as the median (1Q–3Q). The cumulative amount of fentanyl was analyzed through repeated analysis of variance measurements. A chi-square test or Fisher’s exact test were used for the categorical data. The analysis was conducted using SPSS ver. 23.0 software (IBM Corp., USA) and a P value of less than 0.05 was considered statistically significant.
Results
We recruited 42 patients (21 in each group) between April 2016 and March 2017, and all patients received their allocated interventions. One patient in each group was excluded from the final analysis owing to a loss of follow up, and 40 patients (20 in each group) completed the study (Fig. 2). The baseline and perioperative characteristics of the study patients were comparable between the two groups (Table 1). The type of surgery and dose of fentanyl consumed intraoperatively were also similar. Regarding postoperative pain, the VAS at rest 24 h post-block showed no difference between the two procedures; however, the QLB group had lower VAS scores at rest compared with the TAPB group 48 h post-block (Table 2). However, at no point in time were there any differences between the groups in terms of VAS pain scores while coughing. Regarding the postoperative use of analgesics, the cumulative amount of fentanyl and the additional analgesic requirements also showed no differences (Table 3).
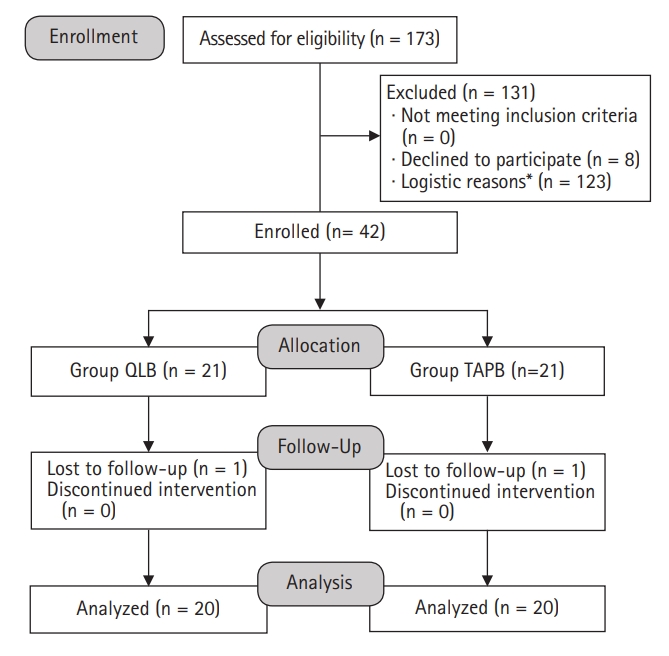
Patient flow diagram. *Researchers were unavailable for the study. QLB: quadratus lumborum block, TAPB: transversus abdominis plane block.
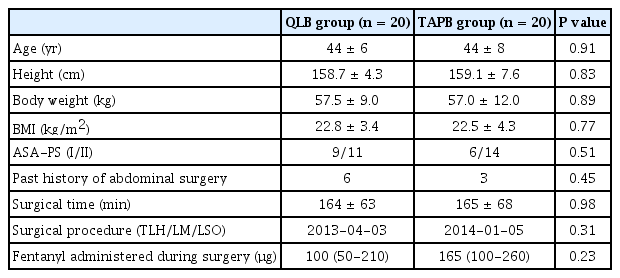
Baseline and Perioperative Characteristics of Study Patients
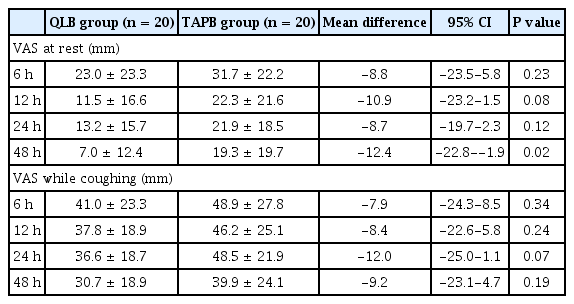
Postoperative Patient Data Regarding Pain and Analgesics
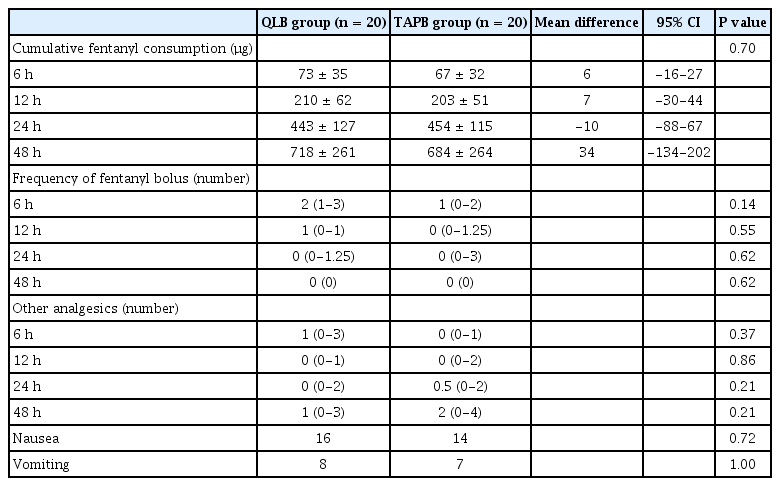
Postoperative Demands for Analgesics and Complications
A sensory blockade was observed at 6 or 12 h after all blocks except for two TAPBs, which were conducted in different patients. The majority of blocks produced a cutaneous sensory blockade in the T11 and 12 dermatomes in both groups (Fig. 3). By contrast, a sensory blockade at T10 was not consistently observed in either group (21 [52.5%] vs. 16 [40.0%] for QLB and TAPB, respectively; P = 0.262). A significantly higher percentage of dermatomes showed a loss of pin-prick sensation in the QLB group as compared with the TAPB group at (13 [32.5%] vs. 0 [0%]; P < 0.001) levels.
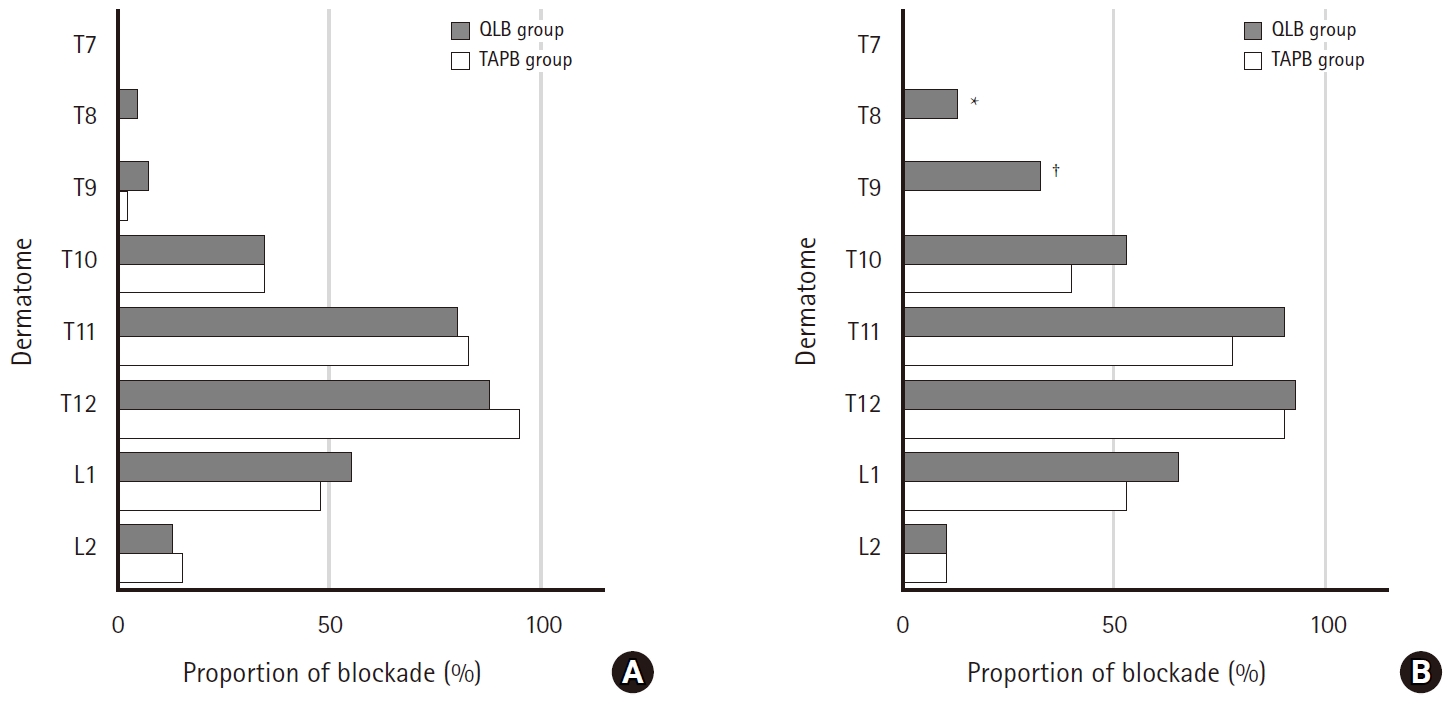
Proportion of sensory blockade at each dermatome observed at 6 or 12 h post-block. Twenty patients received bilateral blocks; therefore, data were collected from 40 blocks for each group. Results are presented as a percentage. (A) Proportion of loss of cold sensation at each dermatome. No significant differences were observed. (B) Proportion of loss of pin-prick sensation at each dermatome. *P = 0.02, †P < 0.001. QLB: quadratus lumborum block, TAPB: transversus abdominis plane block.
The number of dermatomes with a loss of cold and pin-prick sensation, however, was comparable between QLB and TAPB at all time points except for 12 h after block, and decreased as time passed (Fig. 4). Only four (10%) and two (5%) of the blocks were associated with a loss of pin-prick sensation at any dermatome at 48 h after QLB and TAPB, respectively. No block produced a loss of cold sensation lasting 48 h in either group, and none of the patients showed an apparent motor block in the lower leg.
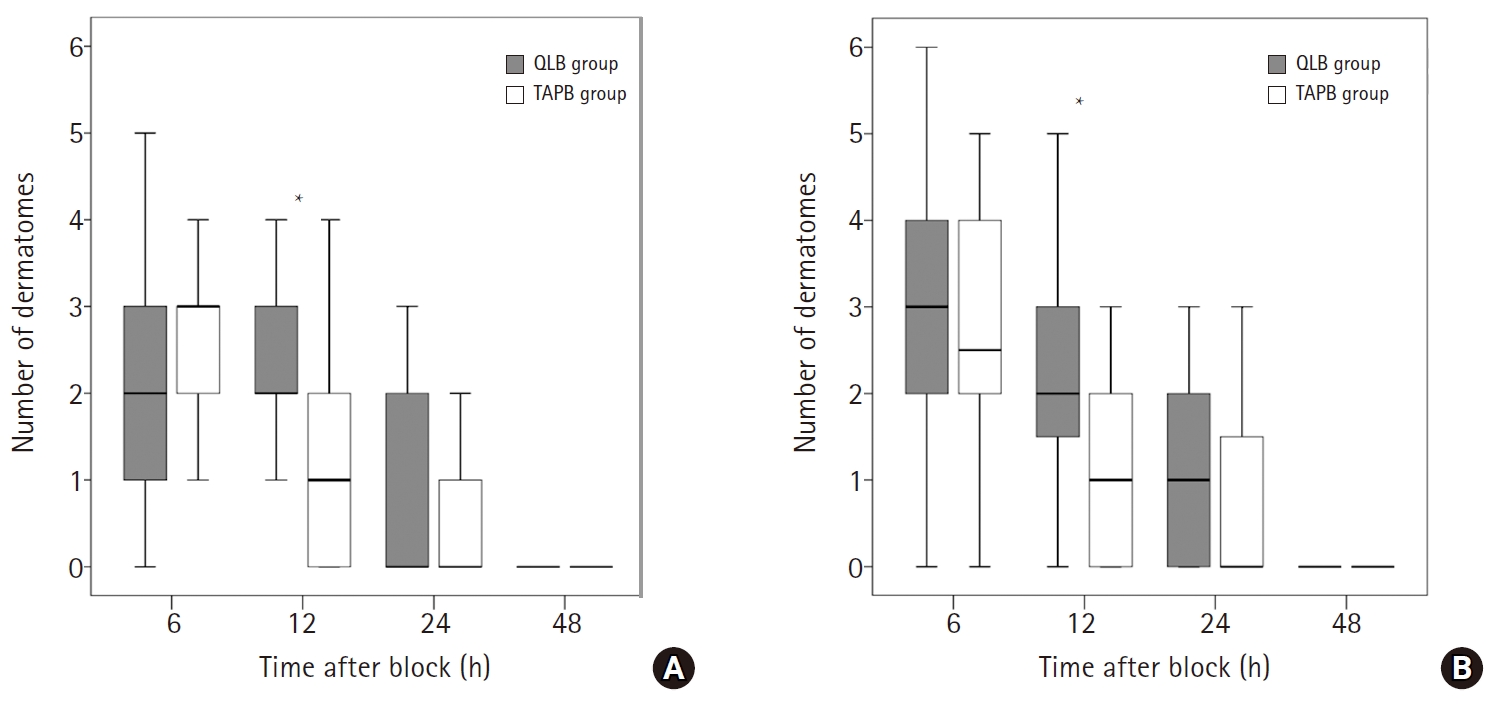
Number of dermatomes with sensory blockade over time. The box represents 1Q–3Q, and the median is represented by the solid line. Error bars above and below the box mark the minimum and maximum values. (A) Number of dermatomes with loss of cold sensation over time. *P = 0.002. (B) Number of dermatomes with loss of pin-prick sensation over time. *P = 0.002. QLB: quadratus lumborum block, TAPB: transversus abdominis plane block.
There were no serious complications attributed to the US-guided blocks, including local anesthetic toxicity or visceral organ injury, in either group. One patient in the QLB group showed hypesthesia in the T12 and L1 dermatomes on postoperative day 3, but completely recovered within 2 days. Postoperative nausea and vomiting occurred similarly between the two groups (Table 3), and the continuous infusion of fentanyl was stopped between 24 and 48 h in six (30%) and five (25%) of the patients in the QLB and TAPB groups, respectively (P = 1.000).
Discussion
In this study, we observed the analgesic effects and distribution of a cutaneous sensory blockade after applying QLB2 and posterior TAPB in patients following laparoscopic gynecologic surgery. During the first 48 h post-block, only a few patients receiving QLB2 or TAPB experienced pain with a VAS of over 60 at rest when using PCA fentanyl. Although the results of the VAS pain scores showed better analgesic conditions at rest with QLB2 than with TAPB at 48 h post-block, the requirements for fentanyl and other analgesics showed no differences between the two groups of patients. The results of a cutaneous sensory assessment showed that a slightly greater cranial spread of the sensory blockade was obtained after QLB2 than that after TAPB; however, only half of the patients developed a sensory blockade over T11 even with QLB2. In addition, the number of dermatomes with a cutaneous sensory blockade was virtually the same between the QLB and TAPB groups.
Since the advent of US-guided peripheral nerve blocks, abdominal wall blocks have become popular, and several different techniques have been introduced. Lateral TAPB was first described by Hebbard et al. [4] and has since been used in numerous institutions. However, this technique has produced limited and inconsistent sensory block and analgesic effects [7,14]. The results of clinical and cadaver studies suggest that the injection site of lateral TAPB may be too anterior or medial, and that a posterior approach may produce more consistent and superior analgesia with the blockade of lateral cutaneous branches of the thoracolumbar nerves [8]. Studies comparing the analgesic effects of posterior and lateral TAPB in patients undergoing a caesarean section [15] or gynecologic laparoscopic surgery [16] have shown the superior analgesic effects of posterior TAPB as compared with those of lateral TAPB.
QLB was first described by Blanco [9] as a technique for injecting a local anesthetic anterior to the quadratus lumborum muscle. The technique was later called QLB1, and thereafter a new approach to QLB using a local anesthetic injected more posteriorly into the LIFT space was introduced as QLB2. The exact mechanism of QLB2 remains unknown. Some studies have claimed that LIFT connects to the middle layer of the thoracolumbar fascia (MTLF), and this plane may allow the injected solution to spread into the paravertebral space where the sympathetic trunks are present. The effects on the sympathetic fibers may also play a role in visceral pain control [10,11].
To the best of our knowledge, this is the first clinical study assessing the distribution of a cutaneous sensory blockade after QLB2 as well as posterior TAPB. Our study results showed that, although some patients demonstrated a loss of cold and/or pin-prick sensation at the T8, T9, and L2 dermatomes, the majority of patients developed a cutaneous sensory blockade only at the T11–T12 level after either blockade. These results are remarkably different from those of studies conducted by Murouchi et al. [17], which showed that the majority of patients developed a loss of cold sensation in T7–T12 dermatomes and in T10–T12 after QLB and lateral TAPB, respectively. However, their technique used for QLB appears to differ from the approach used in the present study; their injection point was inside the epimysium-investing fascia of the quadratus lumborum muscle (Video 2). Although a wider spread of the sensory blockade, i.e., T7–L1, after QLB2 has been reported in some case reports [18,19] and an imaging study [9], previous cadaveric studies have never shown an extensive spread of dye after QLB2 [20,21].
A few clinical studies have compared posterior TAPB and QLB2. Blanco et al. [10] compared TAPB and QLB2 using patients undergoing caesarean section and found that compared with TAPB, QLB reduces the postoperative opioid consumption for up to 48 h. However, their report failed to state exactly whether the TAPB position of injection was either lateral or posterior. In the present study, no reduction was found in postoperative opioid consumption after QLB2 compared with posterior TAPB. When considered along with the afore mentioned results showing a similar sensory blockade in two groups, it is unlikely that QLB2 and posterior TAPB result in extremely different blocks. A recent cadaver study showed that two-thirds of the cases of QLB2 are associated with the spread of dye within the transversus abdominis plane [20]. Because MTLF comprises the aponeurosis of the transversus abdominis muscle and the internal oblique muscle and quadratus lumborum fascia [21], some of the injectate with QLB2 might have worked as posterior TAPB.
The present study has several limitations. First, the patients were not randomly divided because no prior data existed to allow a power analysis to be conducted or to determine the number of patients for the randomized controlled study. Therefore, we alternately conducted either block in order of appearance. Although this was not ideal, we do not believe any bias occurred because 1) no specific pattern was shown in planning the surgery schedule, 2) all blocks were conducted or supervised by the same anesthetist, and 3) measurements were blindly made. If we were to conduct a randomized comparative study using a larger number of patients, we might observe a difference in our primary outcome; for the VAS at rest 24 h post-block, and assuming α = 0.05 and β = 0.2 (80% power), 63 patients were required in each group. However, the difference seems to be small and clinically negligible. Second, in this study, for ethical reasons, we had no control group in which patients would have received sham or no block. Therefore, it is remotely possible that neither block has a beneficial effect on postoperative pain relief. However, the use of no block or a block with saline would not have resulted in a demonstrable sensory blockade. In addition, the efficacy of QLB2 for laparoscopic gynecological surgery has already been shown under different postoperative analgesic regimens [22]. Third, all patients received intravenous fentanyl as a basal infusion postoperatively. Considering the results showing a relatively small number of requests for additional analgesics including bolus fentanyl and relatively low pain scores in both groups, the amount of fentanyl administered as a basal infusion might have obscured the differences between the two groups. Fourth, we only studied female Japanese patients, who are likely less obese than patients in several other countries. Conducting an abdominal wall block in obese patients, particularly in the identification of the injection point for QLB type 2, would be difficult. Fifth, we cannot draw any conclusions regarding the possible difference in duration of the blockade effects between the two blocks because we did not conduct any measurements between 24 and 48 h after the blocks.
To summarize, the analgesic effects of QLB2 and posterior TAPB showed no difference in patients undergoing gynecologic laparoscopic surgery. A cutaneous sensory blockade produced by QLB2 and posterior TAPB was limited to three dermatomal levels in the majority of the patients. However, these findings need to be confirmed through a larger comparative study.
Notes
No potential conflict of interest relevant to this article was reported.
Author Contributions
Yuki Aoyama (Investigation; Formal analysis; Writing-original draft; Writing–review & editing)
Shinichi Sakura (Conceptualization; Investigation; Formal analysis; Supervision; Writing-original draft; Writing–review & editing)
Shoko Abe (Investigation; Data curation; Writing–review & editing)
Minori Wada (Conceptualization; Investigation; Writing–review & editing)
Yoji Saito (Conceptualization; Supervision; Writing–review & editing)
Supplementary Materials
Video 1. Quadratus lumborum block type 2.
The video clip shows quadratus lumborum block type 2, using approach applied in our study. The injection point is within the lumbar interfascial triangle.
Video 2. Intramuscular quadratus lumborum block.
The video clip shows intramuscular quadratus lumborum block where an injection is made inside the epimysium-investing fascia of the quadratus lumborum muscle [17].