Left ventricular aneurysm (LVA) is a common complication of myocardial infarction (MI) [1]. Generally, LVA occurs when a patch of tissue in the ventricular wall rises into a bubble filled with blood. LVA may block passages flowing out of the heart, severely limiting blood flow to the body [1]. Left ventricular false aneurysm (LVFA), on the other hand, is a rare complication following acute MI. LVFA arises from a ventricular free wall rupture that is contained by localized pericardial adhesions. Bleeding is confined to the ruptured space, and fibrous tissue forms around the hematoma to create the false aneurysm [2].
Transmural MI is the most common cause of LVFA and can result from cardiac surgery, trauma and infection [3,4]. Rarely, a LVA may cause LVFA. During MI, LVAs are contained by a layer of muscle. However, if the muscle layer is weakened, a ventricular free wall rupture may occur, forming a false aneurysm. Even when the false aneurysm is small, the rupture risk for an unmanaged LVFA is 30ŌĆō45%, so early surgical resection is recommended [2,4].
We describe a 55-year-old man who was diagnosed via transthoracic echocardiography (TTE), cardiac catheterization, and computed tomography (CT) angiography as having a ventricular aneurysm and false aneurysm that occurred in stage. Given his history of a cerebrovascular accident and cerebellar artery hypoplasia, we focused the surgery anesthesia protocol to avoid hypertensive events and simultaneously to avoid cerebral hypoperfusion. This report presents the successful anesthetic management of this patient.
Case Report
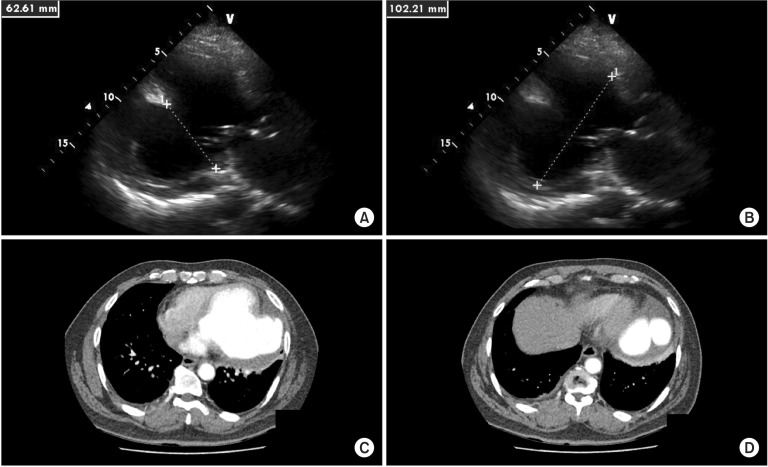
This case report was initiated after obtaining approval from the Institutional Review Board of our hospital. A 55-year-old man (height 169 cm, weight 84 kg) was scheduled for emergency LVA and LVFA resection. His medical history included longstanding hypertension that was controlled with angiotensin-converting enzyme inhibitor, furosemide and a beta-blocker. The patient had sequalae including left-sided hemiplegia after a cerebral hemorrhage of unknown cause and a craniectomy six years previous. About three months before surgery, the patient complained of periodic chest pain, which was considered sequelae from the cerebral hemorrhage. Two weeks before surgery, the patient visited his primary care physician due to exertional dyspnea (NYHA class III), and he was diagnosed as having pulmonary edema, pleural effusion and congestive heart failure (CHF). During management for CHF, he was diagnosed with a large LVA and LVFA and transferred to our hospital for evaluation and management. Chest radiography presented small pericardial and pleural effusion in the right hemithorax. Other laboratory test results were normal, with the exception of increased pro-B-type natriuretic peptide (1,980 pg/ml). We detected an aneurysmal change in the left ventricular (LV) inferior wall, with akinesia of the left circumflex coronary artery territory, using TTE. The LV ejection fraction was 40%, and the LV internal dimension was 102.4 (diastolic)/88.3 (systolic) mm. Pulmonary artery systolic pressure was estimated at 25 mmHg, and grade 1 mitral regurgitation was observed. A large (7 ├Ś 7 cm) aneurysm in the LV lateral wall was observed via CT. The base of the aneurysm had thick wall and it showed contracting shape characteristic of a true aneurysm. However, the apex had a thin wall, bulged with a "snowman" appearance and dilated in the contraction phase, suggesting the possibility of false aneurysm (4 ├Ś 2 cm) (Fig. 1). No evidence of thrombus or rupture was seen in either the true or the false aneurysm on preoperative TTE and CT. CT angiography and brain magnetic resonance imaging (MRI) revealed the extensive previous infarction and postoperative changes in the right middle cerebral artery territory, as well as hypoplasia in the right vertebral artery and extracranial right posterior inferior cerebellar artery. The risk of rupture warranted surgery for surgical resection of the LVFA.
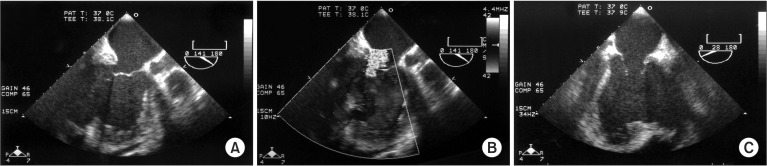
The patient arrived at the operating room with sedative premedication. Standard monitoring using a bi-spectral sensor (Covidien Ilc, Mansfield, MA, USA) and cerebral oximeter (Somanetics, Cerebral Oximeter Invos 5100C, Troy, MI, USA) were applied, and baseline scores were 60% and 50% for the right and left forehead. Initially assessed vital signs (V/S) were stable. Anesthesia was induced with midazolam, fentanyl and etomidate and maintained with a low dose of sevoflurane and high doses of remifentanil and vecuronium for muscle relaxation. We administered fentanyl and midazolam if required. During anesthesia induction, we performed a radial artery catheterization to monitor invasive arterial blood pressure (ABP). Endotracheal intubation with a video laryngoscope (McGrath MAC, Aircraft Medical, Edinburgh, UK) was performed, and mechanical ventilation was initiated with 500 ml tidal volume (TV), 13 per minute respiration rate (RR), 7 cmH2O positive end expiratory pressure (PEEP) and 60% FIO2. During anesthesia induction and endotracheal intubation, V/S was maintained with an ABP of 90/55ŌĆō130/70 mmHg, a pulse rate of around 80 beats/min and a SpO2 of 100%. Arterial blood gas analysis (ABGA) values were pH 7.46, pCO2 38 mmHg and pO2 258 mmHg. We prepared a continuous infusion of dobutamine, phenylephrine and epinephrine to prevent hypotension and nicardipine, nitroglycerine and nitroprusside to prevent hypertension. Trans-esophageal echocardiography (TEE) was performed to evaluate cardiac function and LVFA state (Fig. 2). The LVA and LVFA detected at the inferior LV wall remained unruptured. In several views, there was no filling defect in LVA and LVFA. A mild to moderate degree of mitral regurgitation was suspected due to an enlarged annulus.
Cannulation was performed on the left femoral artery for continuous monitoring of ABP. An 8.5Fr sized introducer (Advanced Venous Access 3Xi, Edwards Lifesciences LLC, Irvine, CA, USA) and Swan-Ganz catheter (Swan-Ganz CCOmbo, CCO/SvO2/CEDV, Edwards lifesciences LLC, Irvine, CA, USA) were inserted under ultrasound guidance into the right internal jugular vein to prepare for the possibility of massive hemorrhage and for continuous monitoring of cardiac output and mixed venous oxygen saturation.
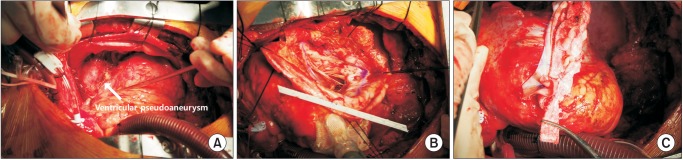
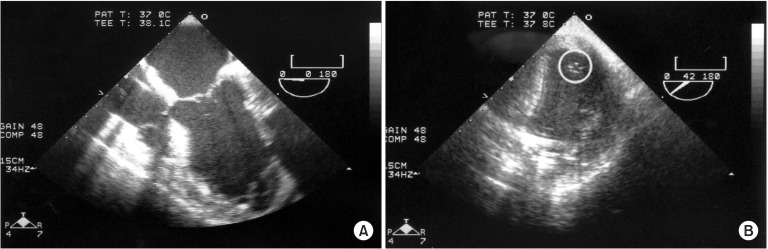
During the operation, our primary hemodynamic goals were to maintain the systolic BP between 100ŌĆō110 mmHg, the diastolic BP between 60 and 80 mmHg, and the pulse rate between 80ŌĆō95 beats/min. To evaluate the cerebral perfusion state, bilateral pupil sizes were compared periodically, and the cerebral oximeter score was maintained between 60% and 70%. Prior to the thoracotomy, we prepared the right femoral area for immediate cannulation for cardiopulmonary bypass (CPB) in the event of LVFA rupture. Following the thoracotomy, sequential partial and total cardiopulmonary bypass and cardiac arrest with hypothermia and hyperkalemic cold blood cardioplegia solution (Choongwae Cardioplergic Solution 1, Korea) were achieved. The LVFA, detected near the apex of the left ventricle, remained unruptured. Surgical resection of the LVFA and infarct area was performed, double-layered bovine pericardium and paricardial patches were applied to support the LV infarct area, and the ventriculotomy was closed (Fig. 3). The aortic clamp time was 83 min, and the total pump time was 103 min. When we attempted CPB weaning, the patient experienced low cardiac output syndrome, likely due to predisposing heart failure and the ventriculotomy. Despite administration of various inotropics and vasoconstrictors, including milrinone (Primaco, Sanofi Winthrop industrie, France; 4.2 mg loading for 15 min, maintained at the rate of 0.4ŌĆō0.7 ┬Ąg/kg/min), dobutamine (DOBUTamine and 5% Dextrose inj., CJ HealthCare Corp., Seoul, Korea; infusion rate 5ŌĆō10 ┬Ąg/kg/min), epinephrine (Epinephrine Daihan Inj. Daihan Pharm Co., Ltd. Seoul. Korea; infusion rate 0.1ŌĆō0.2 ┬Ąg/kg/min) and norepinephrine (Norpin, dalimpharm, Seoul, Korea; infusion rate 0.15ŌĆō0.2 ┬Ąg/kg/min), CPB weaning could not be accomplished. We confirmed ineffective systolic contraction of the LV by TEE (Fig. 4), placed an intra-aortic balloon pump (IABP) and augmented the systemic pressure with a 1 : 1 ratio. After successful CPB weaning, the patient's BP was maintained in the 90/60ŌĆō100/70 mmHg range. At this time, ABGA values were pH 7.26, pCO2 32 mmHg and pO2 289 mmHg with mechanical ventilation; 400 ml TV, 16 /min RR, 10 cmH2O PEEP, 60% FIO2. Cerebral oximeter score changes were 60ŌĆō71% on the left and 56ŌĆō60% on the right during surgery.
Intraoperative fluid management was focused on the surgical procedure and the patient's condition. Especially following CPB weaning, fluid administration was guided by TEE and pulmonary artery pressure. Because the LV was rapidly decompensated with acute volume loading, we minimized crystalloid infusion and transfused blood products on demand. After CPB weaning, the total fluid input was 1,380 ml, and the output was estimated at 965 ml.
One day after the operation (POD 1), the patient's V/S were stable, and IABP support was gradually reduced and ultimately removed. The patient was extubated, and supplementary oxygen was administered through a facial mask. We observed no new onset of neurologic signs or symptoms. Postoperative follow-up TTE showed a marked decrease in LV size, to 56.0 (diastolic)/45.8 (systolic) mm after LVFA resection. Akinesia of the left circumflex coronary artery territory persisted; the LV ejection fraction was 43% on POD 8. Mitral regurgitation was decreased to a trivial level. The patient was discharged from the hospital, without complications, on POD 14.
Discussion
LV free wall ruptures occur in 4% of patients after acute MI and are seen in 23% of patients at autopsy following MI-related death [5]. Immediate cardiac rupture is the cause of death in 7ŌĆō10% of patients with an acute MI [5]. The LVA has a well delineated, thin, scarred, or fibrotic wall because it arises from a weakened ventricular wall due to ischemic injury, and it enlarges over time. The LVFA results from a rupture of the ventricular free wall. The walls of a false aneurysm are composed of an organized hematoma and pericardium and lack elements from the original myocardial wall. Unlike a true aneurysm, a false aneurysm contains no endocardium or myocardium [3]. Therefore, an LVFA has a greater tendency to rupture compared to a true LVA, and ventricular free wall rupture can lead to pericardial tamponade and sudden death [3].
It is difficult to diagnose LVFA because of the absence of precisely defining symptoms [3,5,6]. Patients with LVFA can present with CHF, chest pain and/or dyspnea and sometimes are asymptomatic [3]. TTE, CT, MRI and ventricular angiography can be used for diagnostic imaging [6,7,8,9]. The most reliable method for diagnosing LVFA is angiography, but TTE is a useful first step [2,10,11]. Distinguishing a false aneurysm from a true aneurysm is important because treatment strategies for the two differ vastly. False aneurysms require urgent surgical resection, whereas true aneurysms typically can be managed medically. Unmanaged false aneurysms carry a 30ŌĆō45% risk of rupture, with a mortality of almost 50% reported when managed with medical therapy alone [3]. We initiated immediate surgical treatment for the patient described here due to the large size of the LVFA and the evidence of CHF, which we believed was related to the LVFA and the LVA.
Anesthetic requirements during the LVFA resection included deep anesthesia with high doses of opiates, hypnosis with benzodiazepines and other hypnotic induction agents due to the rupture risk for the LVFA and the ventriculotomy site. However, we also considered that the patient had relative high risk for brain ischemia due to the observed extensive ischemic changes and abnormal perfusion of vessels. Therefore, our anesthetic goal was to maintain marginal upper normal BP to guarantee brain perfusion and to reduce the risk of LV rupture. We maintained a mean arterial pressure between 60ŌĆō70 mmHg to avoid LV rupture and brain hypoperfusion using balanced anesthesia techniques, vasoactive drugs and IABP with hemodynamic monitoring devices and laboratory values including ABGA.
However, deep anesthesia readily produces cardiovascular depression, especially for patients with CHF, when inhalation anesthetics are primarily used. Thus, the patient required meticulous vigilance for hemodynamic monitoring, within a narrow safety range, to anticipate a potential hemodynamic response to high dose opioids and other anesthetics. We observed a slight cardiovascular depression in this patient after even a small additional dose of anesthetic agents. Various invasive hemodynamic monitoring devices, including a Swan-Ganz catheter with mixed venous oxygen saturation, provided information about hemodynamic status. TEE enabled serial inspection of LV preload status and contractile function, and it provided information about the LVFA size and location, the presence of the mural thrombus, and the valvular abnormality [11].
Perioperative anesthetic management of LVFA should be focused on preventing rupture of the aneurysm and on avoiding the risk of vital organ ischemia, which is frequently related to complicated MI events.