Froin's syndrome is characterized by marked cerebrospinal fluid (CSF) xanthochromia (yellow discoloration of the CSF) and hypercoagulability due to increased protein content. The cause of the high protein content of the spinal fluid is meningeal irritation and inflammation. Pseudo-Froin's syndrome has been described as stagnation of the CSF distal to a spinal block due to spinal disc bulging or tumors [1].
A 54-year-old man with paraplegia was admitted to the urology department of our institution for follow-up of a bladder wall malignancy. The patient had suffered from paraplegia for 20 years because of a thoracic spine burst fracture (T5-7) and dislocation. He had undergone operative correction to maintain the curvature of the spine. The patient was currently scheduled for a urinary bladder wall biopsy. At the time of his admission, the patient's vital signs were stable and all laboratory findings including pulmonary function tests and arterial blood gas analysis were within normal limits. Magnetic resonance imaging and computed tomography scans of the brain/spine showed no specific abnormal findings except thoracic spine destruction and dislocation. No motor or sensory abnormalities were found in the upper chest or upper extremities. Because the patient wished to maintain alertness during the operation, it was planned to perform the surgery under spinal anesthesia.
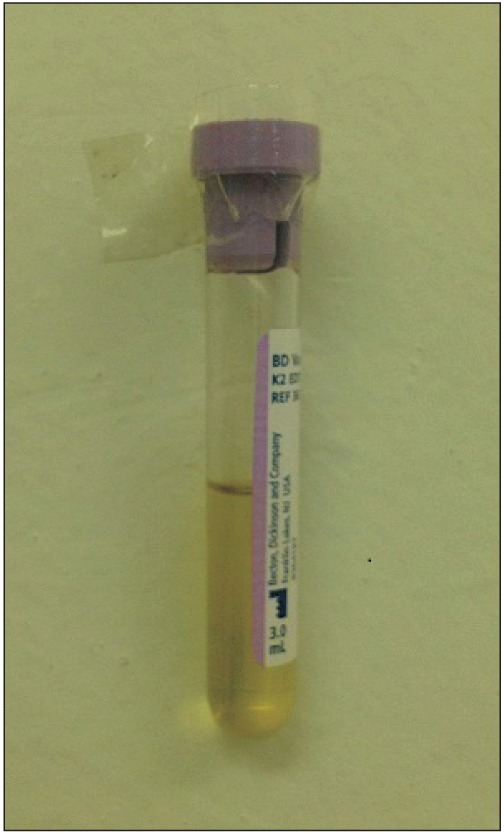
The first time spinal anesthesia was performed, the CSF flow was very scanty and sticky, and the color was dark yellow. "Give" was felt, and the CSF color was judged to be due to a traumatic tap. Spinal drug administration was done after CSF confirmation by aspiration. The patient's mental status and vital signs, especially respiration, were stable throughout the operation following the successful spinal anesthesia. No specific problems such as headache, reflex tachycardia, or sweating were observed in the perioperative period. At the second spinal anesthesia for bladder-cancer follow-up surgery, lumbar spinal pressure was measured. The CSF was observed to not drain freely due to low spinal pressure, below 1 cmH2O, and thick density. The CSF was also observed to be an extraordinarily dark yellow color and very sticky, and CSF was collected by aspiration (Fig. 1). Cell count, cytology, electrophoresis, and culture of the CSF were performed. The CSF studies were performed within 30 min after collection of the fluid. The patient's CSF showed high protein (3,114.5 mg/dl), normal glucose (46 mg/dl) and CSF/blood glucose ratio (0.58), elevated T-cholesterol (31 mg/dl), and triglycerides (5 mg/dl). Cell counts were white blood cells (WBC) 50 cells/µl (neutrophil 45%, lymphocyte 55%) and no red blood cells. Cytology showed atypical cells or malignant unknown cells, but no malignant cells or pathologic organisms were found in culture.
In Froin's syndrome, blockage of the spinal canal and stagnation of the CSF develops due to an obstructing inflammatory or neoplastic lesion. High CSF protein levels are caused by exudation or transudation from a tumor itself or hematogenous factors, in loculated areas of the subarachnoid space, sequestered from cerebrospinal fluid circulation. In Pseudo-Froin's syndrome, high protein levels are also observed in the CSF, and patients complain of back pain and sciatica. Interruption of the spinal canal and stagnation of the CSF by a neoplastic mass or herniated disc contribute to the sequestered CSF circulation and the high protein content of the CSF. Spinal fluid protein can rise to extremely high levels of at least 5 gm/L, as compared to normal levels of 0.15-0.45 gm/L in neurologic disease conditions, such as meningitis or epidural abscess [1]. Causes of a dry tap are blocked needle, needle in the wrong space, spinal surgery, and low CSF pressure. Many trials, including rotating the needle, repeated tapping, position change, and aspiration, should be attempted before spinal drug administration [2]. CSF investigation is required to prove the diagnosis or rule out relevant differential diagnoses. Visual assessment of the CSF color is usually practiced as a means of diagnosing intracranial bleeding, such as subarachnoid hemorrhage, in the neurology department. Spectrophotometric analysis of xanthochromia is recommended for distinction between a traumatic spinal tap and a true intracranial bleed in cases when a yellow color of the CSF is observed. Routine CSF analysis such as total protein, albumin, immunoglobulin, glucose, lactate, cell count, and cytology should be performed immediately after collection [3].
Normal CSF glucose concentration is 50-60% of serum value and a CSF/blood glucose ratio less than 0.4-0.5 is considered pathological. The CSF/blood glucose ratio may be a better single diagnostic indicator, especially in cases of exclusion of bacterial meningitis with no microorganism in the CSF culture [4]. During CSF storage, glucose is degraded, and studies must therefore be performed within 1 hr after CSF collection. High protein contents of the CSF have infectious causes such as bacterial, cryptococcal, or tuberculous meningitis, as well as non-infectious causes, such as subarachnoid hemorrhage, central nervous system (CNS) vasculitis, CNS neoplasm, and autoimmune disease. However, protein and glucose in the CSF are non-specific and not significant, and other parameters are investigated for the diagnosis and prognosis of neurologic disorders. Cholesterol and triglyceride levels in the CSF rise in tuberculous meningitis, pyogenic meningitis, viral encephalitis, and hydrocephalus. Bacterial meningitis is suspected when the WBC count in the CSF exceeds 5 cells/µl and finally diagnosed by identification of pathologic cells in Gram staining or growth of pathogens from CSF culture [3,5].
In the case discussed here, the patient had suffered from 20-year paraplegia with newly-developed urinary bladder cancer and showed abnormal CSF characteristics at spinal anesthesia. Therefore, a tumor of the spine was a suspicious cause of the xanthochromia, and CSF evaluation was performed immediately after CSF collection. The CSF glucose and CSF/blood glucose ratio were normal. Levels of CSF protein and cholesterol were high, but bacterial cells and malignant cells were not found in CSF culture.
Similar to Miraz's case of Pseudo-Froin's syndrome, with a large bulging disc in the lumbar spine, this case showed xanthochromia, high protein content, marked coagulation of the CSF, and dry tapping without spinal meningitis, malignancy, or abscess. This case was concluded to be Pseudo-Froin's syndrome without abnormal neurological findings, simply caused by interruption of CSF flow due to thoracic spine destruction and dislocation.