Is the rapid sequence induction possible with 0.6 mg/kg rocuronium in pediatric patient?
Article information
Abstract
Background
We have investigated the possibility of rocuronium 0.6 mg/kg and timing principle application with the same dose for rapid sequence induction (RSI) in 65 children, aged 4-8 yr.
Methods
Sixty five patients were randomly assigned to one of two groups; Group A (n = 31, timing principle application) received rocuronium (0.6 mg/kg) followed by administration of propofol (2.5 mg/kg), and group B (n = 36) received rocuronium (0.6 mg/kg) after administration of propofol. Intubation was assessed at 60 seconds just after administration of last injectants. Intubating conditions (jaw relaxation, vocal cord movement, and response to tracheal intubation) were evaluated as excellent, good, fair and poor.
Results
Excellent intubation conditions were obtained in 87% in group A and 61% in group B. However, clinically acceptable intubation conditions which means excellent and good did not show any significant difference as 100% (group A) and 99% (group B).
Conclusions
In cases of pediatiric patients undergoing elective surgery, RSI was possible irrespective of the use of timing principle.
Introduction
Rocuronium is a steroidal, non-depolarizing muscle relaxant with a prompt action time, and it has been introduced as a drug whose intubation condition is similar to that of succinlycholine. Accordingly, rocuronium has been proposed as a drug which can be alternatively used to succinlycholine with the advantage of a lack of the side effects of succinlycholine. According to recent studies which have been conducted in adults, it was assessed to have an equivalent profile of the intubation condition to succinlycholine or suxamethonium [1-4].
According to Naguib et al. [5], following a comparison of the endotracheal intubation condition within 60 seconds following the induction of anesthesia in children, rocuronium 0.9 mg/kg was equivalent to suxamethonium 1 mg/kg. Besides, according to Mazurek et al. [6], an endotracheal intubation could be performed using rocuronium 1.2 mg/kg within 60 seconds in a similar manner to suxamethonium 1.5 mg/kg. In cases of surgery which was completed within an hour, however, rocuronium 1.2 mg/kg would be relatively higher. This long action time may cause unfavorable complications. In particular, in pediatric patients or those who underwent a daily surgery whose frequency has recently been increasing, it can be considered as inappropriate. Accordingly in pediatric cases in which approximately an hour elapsed for surgery, if RSI should be possible at a dose of rocuronium 0.6 mg/kg, this would be very ideal. According to Cheng et al. [7], however, in pediatric cases in which a modified RSI was performed, rocuronium 0.9 mg/kg had an equivalent profile of endotracheal intubation condition to suxamethonium 1.5 mg/kg. But these authors noted that rocuronium 0.6 mg/kg would be inappropriate.
At a dose of common types of non-depolarizing muscle relaxant, as the methods for shortening the time of action, there are a priming principle where 20% of a 1.5-time dose of ED95 is administered 2-4 minutes prior to an endotracheal intubation [8], those in which an optimal dose of ephedrine is used [9] and the timing mechanism where changes are made for the time point for the intravenous infusion of rocuronium [10]. Nelson et al. [10] reported that rocuronium 0.6 mg/kg could produce an equivalent profile of the intubation condition to RSI when applied with timing principle in adults which is similar to a succinylcholine 1 mg/kg.
Given the above background, to examine whether RSI could also be performed using a dose of rocuronium 0.6 mg/kg in pediatric patients, a comparison was made between cases in which a timing principle was used and otherwise cases.
Materials and Methods
Following the approval from institutional review board, through a preoperative visit, an informed consent was fully obtained for general anesthesia and the current study. A written informed consent was obtained from subjects. The current study was conducted in 67 pediatric patients aged 4-8 years who corresponded to physical grade 1 of The American Society of Anesthesiology and then underwent endotracheal intubation under general anesthesia. In cases in which the surgical time was much shorter, i.e., within 30 minutes, patients with upper respiratory infection or asthma, those in whom a difficult endotracheal intubation was expected, those with muscular dystrophy and those with a past history of allergy to the drugs which are used during anesthetic induction were excluded from the current analysis. Types of surgery which patients underwent include strabismus, orchiopexy, appendectomy, myringotomy and tendon injury. For pre-medications prior to anesthesia, pethidine 1 mg/kg was intramuscularly injected at 30 minutes prior to an entry into an operation room. Following this, an electrocardiography (ECG), a non-invasive blood pressure monitoring and pulse oximeter were implanted in patients. Using a venous route which was maintained in a ward, 1 : 2 sodium dextrose solution 500 ml was slowly intravenously infused. In a stable condition prior to anesthetic induction, changes in mean arterial pressure and heart rate were recorded.
In accordance with the methods for administering rocuronium, patients were assigned to two groups as shown below:
(1) The group A (n = 31) where rocuronium (0.6 mg/kg) was intravenously infused and propofol (2.5 mg/kg) was administered 20 seconds later.
(2) The group B (n = 36) where propofol (2.5 mg/kg) was intravenously infused for 10-20 seconds and this was followed by a sequential administration of rocuronium (0.6 mg/kg).
At this time, in all the groups, to reduce the pain occurring as a result of the intravenous infusion of propofol or rocuronium, lidocaine (1 mg/kg) was mixed with the drug which was first infused. Then, this mixture was intravenously infused. Following anesthetic induction, prior to an endotracheal intubation, a facial mask was used to perform a manual respiration with the use of 100% O2 3 L.
As the time point for endotracheal intubation, in both the groups A and B, an endotracheal intubation was performed within 60 seconds following the administration of final drugs. An anesthetic induction was performed by specialists in pediatric anesthesia. An endotracheal intubation was performed by a resident with a more than 3-year experience who was blinded with which groups comprised the corresponding patients. Then, an endotracheal intubation condition was assessed. Following an endotracheal intubation, with the use O2 1.5 L/min, N2O 1.5 L/min and sevoflurane 2.0 vol%, an anesthesia was maintained. Prior to endotracheal intubation and at 1, 2 and 5 minutes following it, heart rate and mean arterial pressure were measured.
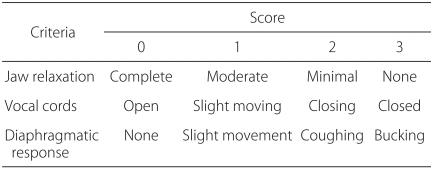
As outcome measures, a comparison was made for the environment for endotracheal intubation within 60 seconds following an intravenous infusion of rocuronium (the degree of mandibular relaxation, vocal cord movements and diaphragmatic response). At this time, for an assessment of the environment for endotracheal intubation, each category was scored with 0-3 points and the scores obtained from four categories were summed. The environment for endotracheal intubation was assessed as very excellent (0-1 points), excellent (2-3 points), fair (4-6 points) and poor (7-9 points).
In the current study, all the measurements were expressed as mean ± SD (SD: standard deviation). A statistical analysis was performed using SPSS 14.0 (SPSS Inc., USA).
Between the two groups, a comparison of age, sex and weight was made using an unpaired t-test. Such demographic statistics as the type of surgery, the environment for endotracheal intubation and the degree of muscle relaxation were compared between the two groups using Fisher's exact test. A value of P < 0.05 was considered statistically significant.
Result
To evaluate the environment for endotracheal intubation, such outcome measures as the degree of mandibular relaxation, the movement of vocal cords and the diaphragmatic response were scored with 0, 1, 2 and 3 points (Table 1).
Assessment of Intubation Conditions
Patients of both group showed a similar distribution of disease (Table 2).
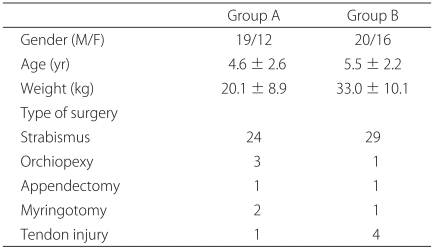
Demographic Data
Following a comparison of the environment for endotracheal intubation, an endotracheal intubation which was very excellent from a clinical perspective was found to be in 87% (27/31) of the group A and 61% (21/34) of the group B.
In particular, the environment for endotracheal intubation whose score was lower than 3 points, including very excellent cases and excellent cases, was found to be in 100% (31/31) of the group A. This indicates that all the subjects had more than very excellent environment for endotracheal intubation. In the group B, it was seen in 99% (34/36). Scores indicating the environment for endotracheal intubation were found to be 0.4 ± 0.8 in the group A and 0.5 ± 0.5 in the group B (Table 3).

Intubation Conditions
Discussion
As a result of the current study, at a dose of rocuronium 0.6 mg/kg, in both the group A where a timing principle was applied and the group B where no timing principle was applied, RSI could be performed. In particular, of the environments for endotracheal intubation, group A showed 'very excellent' in 27 patients (87%). This figure was much greater than the group B, but there was no statistical significance.
Unlike adults, pediatric patients are more sensitive to the side effects occurring following the use of succinylcholine. Accordingly, its use has been decreased [11]. For this reason, there are various methods for expressing the prompt actions of non-depolarizing muscle relaxant which could be alternatively used to succinlycholine. Of non-depolarizing muscle relaxants which are frequently used at the present, rocuronium has been favored because of a prompt action time. Both the action time and persistent time have a dose-dependent property. In other words, if RSI should be performed to such an equivalent extent to succinylcholine, the dose of rocuronium 0.9-1.2 mg/kg is required [1]. In cases in which the above dose is used, due to the prolongation of muscular relaxation, there may be an effect on the persistence time and recovery. Accordingly, we used the methods for intravenously infusing based on a timing principle as the attempts to improve the conditions for endotracheal intubation using a minimal dose of rocuronium in pediatric patients. Both methods showed very excellent environment for endotracheal intubation. According to Fuchs-Buder et al. [12], a comparison of the degree of muscle relaxation depending on the environment for endotracheal intubation and time was made at two doses of 0.6 mg/kg and 0.9 mg/kg in pediatric patients. These authors noted that clinically excellent RSI could be performed at both doses. In a study which was conducted by Fuchs-Buder et al. [12], when a dose of 0.6 mg/kg was infused, without using a timing principle, alfentanil 10 mcg/kg was alternatively used for anesthetic induction. The environment for endotracheal intubation was shown to be very excellent in 29/35, excellent in 6/35, fair in 0/35 and poor in 0/35. This pattern of distribution was very similar to cases in which a timing principle was used in the current study. In these studies, through a time-dependent monitoring of the muscle relaxation, the action time was measured. The actual action time was 193 seconds (rocuronium 0.6 mg/kg) and 118 seconds (rocuronium 0.9 mg/kg). This was close to vecuronium. Within a minute, however, excellent environment for endotracheal intubation could be obtained. This is not only because a lag time (the time elapsed until a decreased twitching height was noted since the infusion) following the infusion of rocuronium (the time elapsed until a decreased twitching height was noted since the infusion) was approximately 30 seconds but also because the degree of muscle relaxation was relatively higher following the infusion of rocuronium.
To accelerate the action of non-depolarizing muscle relaxant, there are such methods as priming principle or timing principle. In association with this, according to Bock et al. [13], in cases in which a priming principle was used, at a dose of 0.6 mg/kg, the excellent environment for endotracheal intubation and a prompt action time could be obtained. According to Tryba et al. [14], however, a priming principle could not improve the environment for endotracheal intubation in cases in which an endotracheal intubation was performed 60 seconds later using rocuronium. In cases in which rocuronium was intravenously infused prior to the infusion of induction agent, however, the environment for endotracheal intubation could be improved. And they reported that a timing principle was the only useful method by which RSI could be performed using a minimal dose of rocuronium. The same priming principle was used in studies which were conducted by Bock et al. [13] or Tryba et al. [14]. But these authors presented the contradictory results. The reasons are that there was a difference in the subject patients. In other words, the sensitivity to muscle relaxants was increased in pediatric patients as compared with adult patients. For this reason, this difference seen in the subject patients was responsible to some extents. Nelson et al. [10] also classified patients into the group where rocuronium 0.6 mg/kg was administered based on a timing principle and that succinylcholine 1 mg/kg was intravenously infused in a sequential manner. According to these authors, the action time of muscle relaxants was significantly shorter in the succinylcholine group. But there was no significant difference in the environment for endotracheal intubation between the two groups.
In cases in which a timing principle was used, a clinical weakness of the muscle strength rather than a loss of the consciousness preceedingly occur. Accordingly, patients can perceive the discomfort during the anesthetic induction. Sieber et al. [15] intravenously infused rocuronium 0.6 mg/kg using a timing principle during the anesthetic induction. Then, as the sign of muscle weakness, patients' ptosis was confirmed. Following this, induction agent was infused. In cases in which a questionnaire survey was conducted in association with the induction of anesthesia, however, there were no cases of discomfort. They sufggested that, the possible reasons might be that fentanyl and midazolam were preoperatively administered. The time points for the occurrence of clinical muscle weakness include 32 ± 4.9 and 32 ± 5.3 seconds. As the scope is very narrow, the muscle relaxants should be first administered. Until a ptosis occurs, without waiting, the administration of venous anesthetic inducers after 20 seconds is recommended. In other words, a fixed length of time of 20 seconds is recommended. In accordance with this, we did not observe the clinical signs of muscle weakness following the infusion of muscle relaxants. We used the methods for infusing the induction agent following a fixed length of time.
Another method for accelerating the action of non-depolarizing muscle relaxants is to shorten the action time of rocuronium using an optimal dose of ephedrine [16]. This is due to the effects of cardiac output and drug circulation time in response to the action time of muscle relaxants [17]. According to Munoz et al. [18], using an appropriate dose of ephedrine, the action time of rocuronium was shortened from 98 seconds to 72 seconds. By contrast, Szmuck et al. [16] noted that the action time of rocuronium was prolonged in cases in which esomlol was used.
In the current study, the action time of muscle relaxants, which is expected to have a relationship with the environment for endotracheal intubation, was not measured. A measurement of the action time in defining the appropriate environment for endotracheal intubation remains controversial. As a matter of fact, according to Agoston [19], the action time of muscle relaxants was overestimated as a prognostic indicator for the appropriate environment for endotracheal intubation and it is an insignificant factor in defining an appropriate environment for endotracheal intubation. Besides, using a nerve stimulator, the degree of the relaxation of adductor pollicis muscle was assessed. But there was a lesser extent of the correlation between the environment for endotracheal intubation and the degree of the relaxation of adductor pollicis muscle. In association with this, according to Viby-Mogensen et al. [20], at the time point when a complete relaxation of adductor pollicis muscle was observed, the methods for measuring the time and condition for endotracheal intubation were inappropriate. These authors noted that further studies are warranted to examine whether adductor pollicis muscle is appropriate for monitoring the relaxation of muscles.
In planning the current study, we speculated that RSI could not be performed through a single use of induction agents and rocuronium 0.6 mg/kg without additional use of opioids.
Accordingly, we applied a timing principle to the current study. In a different manner to what we expected, however, in both the group where a timing principle was applied and the group where no timing principle was applied, the environment for endotracheal intubation which was clinically excellent could be obtained. The reasons are as follows:
(1) The degree of muscle relaxation was relatively higher in the early stage following the infusion of rocuronium [11].
(2) Subjects patients were pediatric cases aged 4-8 years old, and these patients were sensitive to muscle relaxants differently from adults.
In conclusion, at a dose of rocuronium 0.6 mg/kg, with no respect to the application of a timing principle, RSI could be performed. Because the current study was conducted in patients who were supposed to undergo elective surgery, however, its results cannot be generalized to pediatric patients in an emergency care setting.