Introduction
The use of opioid-based intravenous-patient controlled analgesia (IV-PCA) for controlling postoperative pain has become widespread. Yet while IV-PCA is effective in controlling postoperative pain, continuous administration of opioid can cause or aggravate postoperative nausea and vomiting (PONV).
PONV, like postoperative pain, is a complication that delays recovery, prolongs hospital stays, and increases costs due to additional drug use [1]. PONV is the most common reason why patients choose to stop IV-PCA.
Thus there have been many studies on methods and drugs to prevent PONV. The 5-Hydroxytryptamine (5-HT3) receptor antagonist is being commonly used because it is more effective in PONV prevention and treatment than other antiemetics and has few side effects [2]. Among 5-HT3 receptor antagonists, ondansetron is the most widely used drug, granisetron and ramosetron are also used. Recently, palonosetron has been reported to be effective against chemotherapy-induced nausea and vomiting [3,4] and effective in the prevention of PONV [5,6].
Palonosetron is a newly developed 5-HT3 receptor antagonist. Its receptor-affinity is more potent than other antagonists. Its plasma half-life is very long [7,8], Also it is known to be more effective than ondansetron against nausea and vomiting in patients using anticancer drugs [4]. However, studies comparing the effects of preventing PONV between palonosetron and other 5-HT3 receptor antagonists are sparse.
Thus we compared the effects of palonosetron and ondansetron in PONV prevention in patients who underwent laparoscopic gynecological surgery and used IV-PCA after surgery.
Materials and Methods
The subjects of the present study were 100 American Society of Anesthesiologists physical status I and II female non-smoker patients aged 18 years and above, scheduled for gynecological laparoscopic surgery, with no history of PONV or motion sickness. Patients were excluded from the study if they had diseases in the major organs, were pregnant, vomited or taken antiemetics within 24 h before surgery, or if they were allergic to the study drugs. We launched the prospective study upon receiving approval from the Institutional Review Board of the Presbyterian Medical Center, Jeonju, North Jeolla Province, Republic of Korea and received informed consent from the patients.
All patients were kept in the NPO state for 8 h or longer. The patients did not receive premedication. General anesthesia was induced with propofol 1.5-2 mg/kg and remifentanil 1 ┬Ąg/kg. Tracheal intubation was facilitated with rocuronium 0.8-1 mg/kg. Anesthesia was maintained with sevoflurane 1.5-3 vol%, O2-N2O 3 L/min (FiO2 0.5), and remifentanil 0.05-0.1 ┬Ąg/kg/min. Heart rate and blood pressure were kept in the 20% range of base-line before anesthesia. Mechanical ventilation was performed so that PETCO2 was 30-35 mmHg. When the surgery was over, pyridostigmine and glycopyrrolate were used for reversing muscle relaxation. The patient was extubated with the return of consciousness and the stabilization of spontaneous breathing.
The patients were randomly assigned to the ondansetron group (n = 50) and the palonosetron group (n = 50). In the ondansetron group, ondansetron 8 mg (4 ml) was i.v. administered as a bolus injection immediately before anesthesia induction. Ondansetron 16 mg (8 ml) was added in IV-PCA and was continuously infused. In the palonosetron group, palonosetron 0.075 mg (4 ml) was i.v. administered immediately before anesthesia induction and normal saline 8 ml was added to the IV-PCA. In both groups, fentanyl 600 ┬Ąg and ketorolac 240 mg were diluted with normal saline 100 ml. The basal rate for IV-PCA was 2 ml/h, bolus injection was 2 ml, and the lockout time was set at 15 min. Both groups used identical syringes for bolus intravenous injection and the same type of IV-PCA machine. Fifteen min before the end of the surgery, continuous intravenous administration of remifentanil was discontinued and IV-PCA was infused. After the surgery, if the patient wanted additional analgesics, ketorolac 30 mg was given.
2 h after the surgery (recovery room), 24 h, 48 h, 72 h, an anesthesiologist, blinded to group assignment, visited the patients and assessed whether or not the patients had nausea and vomiting. Nausea was defined as a subjectively unpleasant feeling associated with the awareness of the urge to vomit. Vomiting was defined as an actual physical phenomenon of the forceful expulsion of gastric contents from the mouth. Retching was defined as labored, spasmodic contractions of the respiratory muscle without expulsion of gastric contents. If the patient retched and had the symptoms of vomiting, it was counted as vomiting. Side-effects of 5-HT3 receptor antagonists, which are headache, dizziness, drowsiness were also evaluated. If the patient wanted treatment for continuous PONV, metoclopramide 10 mg was additionally i.v. administered.
For the sample size for the two groups, the power was set at 80% (╬▓ = 0.2) with a 30% reduction of PONV incidence. The significant level was set as 5% (╬▒ = 0.05, two-tailed). The calculated sample size was minimum 42, so taking potential drop-outs into consideration, the sample size was set as 50 for each group [5,9].
SPSS 14.0 was used for statistical analysis (SPSS, Inc, an IBM Company, Chicago, Illinois, USA). The patients' age, height, weight, and anesthesia time were analyzed using the independent t-test. The incidence of PONV was analyzed using chi-square test and Fisher's exact test. Null hypotheses of no difference were rejected if P values were less than 0.05.
Results
The study enrolled 100 patients until completion with no drop-outs.
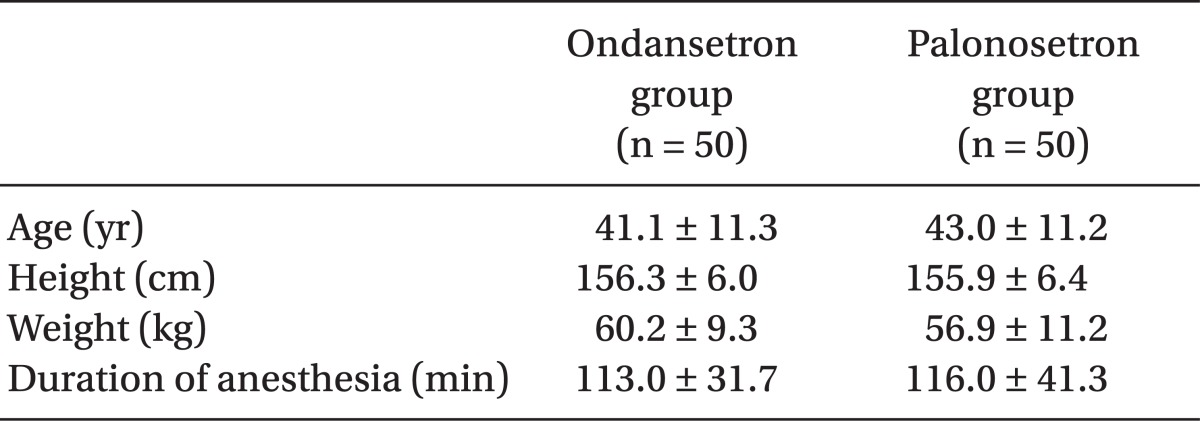
There were no significant differences between the two groups in patient characteristics and anesthesia time (Table 1).
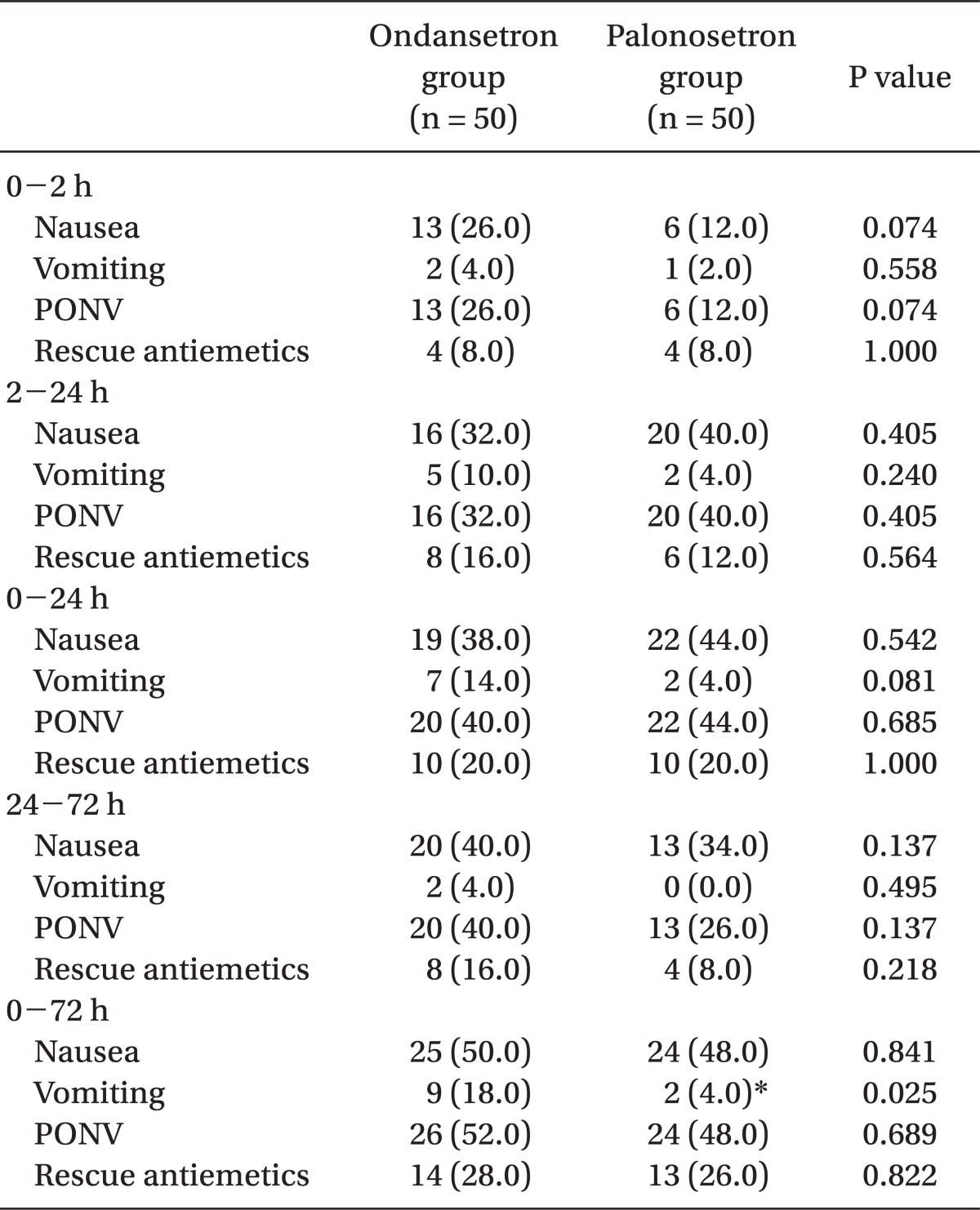
The PONV incidence rates for each of the set times were similar in the two groups. There was no difference in the total incidence rates of PONV in 0-72 h (52% for the ondansetron group, 48% for the palonosetron group). The incidence rate for vomiting was significantly lower in the ondansetron group than the palonosetron group (18% vs. 4%, P = 0.025). There was no difference in the use of additional antiemetics between the two groups (Table 2).
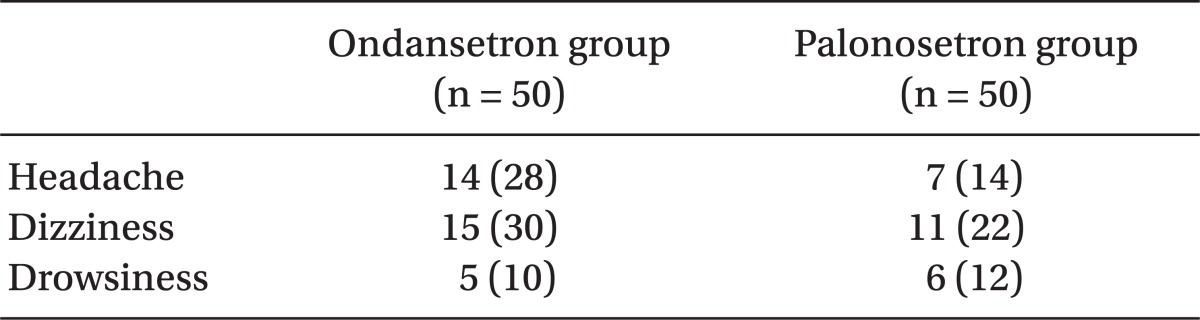
There were postoperative side-effects such as headache, dizziness, and drowsiness, but they did not differ significantly between the ondansetron group and the palonosetron group (Table 3).
Discussion
PONV is a complication that causes discomfort and dissatisfaction in patients who undergo surgery. There are many methods for its prevention and treatment. Nevertheless the incidence rate of PONV is 20-30%. It is affected by factors related to surgery, anesthesia, and the patient [1]. Apfel et al. [10] stated that among patients receiving inhaled anesthesia, female, a history of PONV or motion sickness, non-smoker, and postoperatively using opioid were the more important risk factors of PONV, and each additional risk factor increased the PONV incidence rate to 21, 39, 61, and 79%.
The boundary of the present study was restricted to female non-smoker who used opioids for IV-PCA. These patients belonged to the high risk group since they had three of the risk factors listed by Apfel et al. [10] and had laparoscopic surgery, which is known for a high incidence of PONV. So they were expected to have a high PONV incidence rate [11,12]. Thus on an ethical reasons, the study did not include a control group.
Opioid-based IV-PCA is a safe method for managing postoperative pain with a high rate of satisfaction because the patient self-infuses additional doses when necessary and keeps the drug's plasma concentration stable [13]. However, postoperative opioid use had caused PONV in many studies [10]. When PONV occurs while using IV-PCA, patients do not infuse adequate doses for pain control [14]. Sometimes patients voluntarily stop PCA, so antiemetics are used for PONV prevention.
Many types of 5-HT3 receptor antagonists are being currently used to prevent PONV. It affects the receptors of 5-HT3 in the mucous membrane of the stomach and the central chemoreceptor trigger zone and suppresses nausea and vomiting. Among them, ondansetron is the most widely used type [15].
Palonosetron is a second generation serotonin 5-HT3 receptor antagonist. Unlike other antagonists, it has unique structural, pharmacological, clinical characteristics. Other antagonists directly compete with serotonin, but palonosetron has an indirect effect by its allosteric binding with 5-HT3 receptors [16]. Also it suppresses the response induced by substance P, has negative cooperativity with neurokinin-1 receptors by cross-talk, and creates an antiemetic effect [17]. These explain strong receptor-affinity of palonosetron and its long plasma half-life.
In high-risk groups for PONV such as in the present study, combination treatments such as TIVA with propofol and other drugs are recommended [18]. However, the present study aimed at comparing the effects of two drugs, so combination preventive methods could not be used. Instead, extensive literature was reviewed to find and use the method that best prevents PONV [5,6,9,19-21]. There have been many studies on optimal dose and usage of ondansetron. Generally an iv. injection of 8 mg is suggested as appropriate [19]. There are reports that when using opioid-based IV-PCA, adding ondansetron decreases PONV [20,21]. Palonosetron 0.075 mg is reported to be more effective in PONV prevention than 0.025 mg and 0.050 mg [5,6]. The findings of the studies above were collated so that in the present study, ondansetron 8 mg was infused as a bolus and 16 mg was added to IV-PCA and continuously infused. Palonosetron 0.075 mg was infused as a bolus.
Recently there have been studies comparing the effects of palonosetron and other 5-HT3 receptor antagonists on PONV prevention [22-24]. Park and Cho [22] studied the use of ondansetron 8 mg and palonosetron 0.075 mg before anesthesia induction on patients with two or more risk factors. Palonosetron (42.2%) was far better than ondansetron (66.7%) in PONV prevention up to 24 h. Moon et al. [23] compared the effects of ondansetron and palonosetron in PONV prevention in high-risk patients with three or more risk factors. Similar to the present study, ondansetron was added to IV-PCA. As a result, palonosetron was far more effective than ondansetron in PONV prevention for 2-24 h (42% vs. 62%). However, in the present study the PONV incidence rates were similar in the palonosetron group (48%) and the ondansetron group (52%). But similar to the preventive effects found in other studies, the PONV incidence rate up to 24 h for the palonosetron group was 44%. In the present study, the method used in the ondansetron group (which used 8 mg as i.v. bolus and continuous iv. infusion of 16 mg addition in IV-PCA) was noteworthy in its remarkable effect in PONV prevention.
Palonosetron, as a 5-HT3 receptor antagonist, also has side-effects such as headache, dizziness, and drowsiness. In the present study the two groups showed no difference in the incidence of side-effects. Recently the US FDA has warned against the use of ondansetron, which like droperidol, can cause severe heart complications such as QTc interval prolongation. But palonosetron is not known to have such severe side effects [7].
For ethical reasons, this study did not include a control group using placebos for high-risk patients for PONV. Thus the present study is limited in the sense that it could not defind the base incidence rate for PONV in this particular procedure. Another limitations of the present study is that equipotent doses of the two drugs were not used; instead optimal doses were used for comparisons. For further study, these limitations need to be addressed and many other methods should be used with a large patient size.
In conclusion, bolus of palonosetron 0.075 mg had preventive effects on PONV similar to a bolus of ondansetron 8 mg and continuous i.v. administration of an addition of ondansetron 16 mg in the IV-PCA in high-risk patients who were using IV-PCA after gynecological laparoscopic surgery.