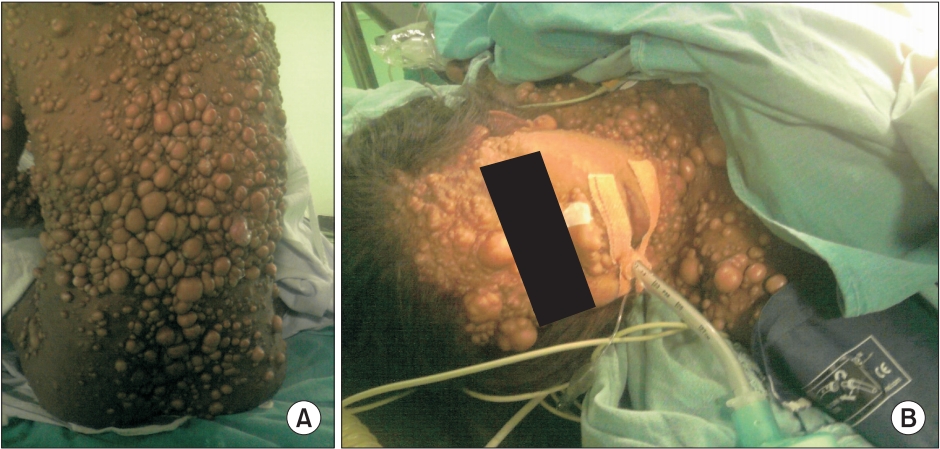
Anesthetic considerations in cases of von Recklinghausen neurofibromatosis differ with varying severity of systemic involvement [1]. After taking written consent of the patient for possible publication of her case in medical literature, we are reporting case of Von Recklinghausen neurofibromatosis in a 55-year-old female, operated for hysterectomy for dysfunctional uterine bleeding, having extensive nodular neurofibroma all over the body (Fig. 1A). Systemic examination revealed normal airway, moderate restrictive lung disease, moderate hypertension, and normal screening magnetic resonance imaging of the brain and spine.
General anesthesia was administered as per standard protocol except for reduced doses of non-depolarizing neuromuscular blocking agent (NdNMBA) along with neuromuscular monitoring (Fig. 1B). Intraoral airway was normal and neck extension was minimized to prevent the cervical spine injury during laryngoscopy. Peri-operative period remained uneventful except for increased sensitivity to vecuronium and residual muscle paralysis in post-anesthesia care unit (PACU) even after administering required doses of neostigmine for reversal of NMBA. In the PACU, the patient had to be supported with invasive ventilation for maintaining adequate minute ventilation for two hours without any further complications.
Neurofibromatosis is an autosomal dominant disease of the ectodermal and mesodermal tissue with varying incidence and severity of involvement of all organ systems. General anesthesia is preferred over regional anesthesia owing to a number of reasons, but if intraoral pathology is suspected, regional techniques should be adopted. Richardson et al. [2] recommended no reduction in doses of NdNMBA after a retrospective review of data of anesthetized Von Recklinghausen neurofibromatosis patients. Nevertheless, keeping the patient euthermic by active heating and use of neuromuscular monitoring is a prudent approach to avoid residual muscle paralysis [1]. However, rarely encountered, Von Recklinghausen neurofibromatosis poses a fundamental challenge in the decision making of the perioperative care provider for improved outcome of the patient.