Introduction
Trauma is notoriously associated with coagulopathy. Primarily, hemostatic impairment can be caused by the trauma itself, as described by Hess et al. [1] as "trauma-induced coagulopathy" (TIC). However, 25ŌĆō85% of patients admitted to trauma centers are additionally intoxicated. In particular, vehicle accidents are often associated with alcohol consumption [2-5]. As alcohol alters coagulation, its effects might have far-reaching implications for trauma patients [6-8].
Previous studies showed multiple alterations in platelet function and prolonged bleeding time [9], inhibition of platelet adhesion to fibrinogen [10], impairment of fibrinolysis [11-13], slower rates of fibrin formation and fibrin cross-linking [3], and reduced fibrinogen and fibrin functionality [10,13]. A study found no effect on standard coagulation measures and no hemorrhagic complications [14]. Nonetheless, the precise in-vivo effects and temporal correlations of ethanol on hemostasis are still poorly understood.
While the prognostic relevance of ethanol levels in trauma remains unclear [15,16], the strong correlation between compromised blood coagulation and a worse outcome after trauma indicate the possible effects of ethanol consumption on clinical outcome [17,18]. Trauma mortality increases with blood ethanol level [19,20] and is associated with increased blood loss, resulting in a need for volume resuscitation and red blood cell transfusion [21]. Consequently, precise knowledge and specific treatment of hemostatic impairment caused by ethanol may be crucial.
Conventional coagulation tests are restricted to certain stages and components of the clotting process and, thus, neglect clot characteristics and possible hyperfibrinolysis. Hence, many trauma centers routinely apply viscoelastic point-of-care tests such as rotational thromboelastometry (ROTEM) for a more detailed hemostatic evaluation, as it reliably differentiates platelet or fibrinogen dysfunctions and also detects hyperfibrinolysis.
In a ROTEM based in-vitro study, Engstr├Čm et al. [11] demonstrated a prolonged clot formation time (CFT) of 34% at an ethanol concentration of 1ŌĆ░. At an ethanol concentration of 4ŌĆ░, they found a prolonged CFT of about 118% as well as significantly reduced fibrinolysis.
We, therefore, examined the possible in-vivo hemostatic effects of ethanol through ROTEM in non-traumatized healthy volunteers.
Materials and Methods
This study was reviewed and approved by the local ethics committee at Hannover Medical School (No. 2066-2013).
Participants
We used the results from Engstr├Čm et al. to calculate the required sample size. Based on the reported change in CFT of about 34% at an ethanol concentration of 1 ŌĆ░, a power of 80%, and a significance level of 0.05, 19 patients were required for sufficient evaluation.
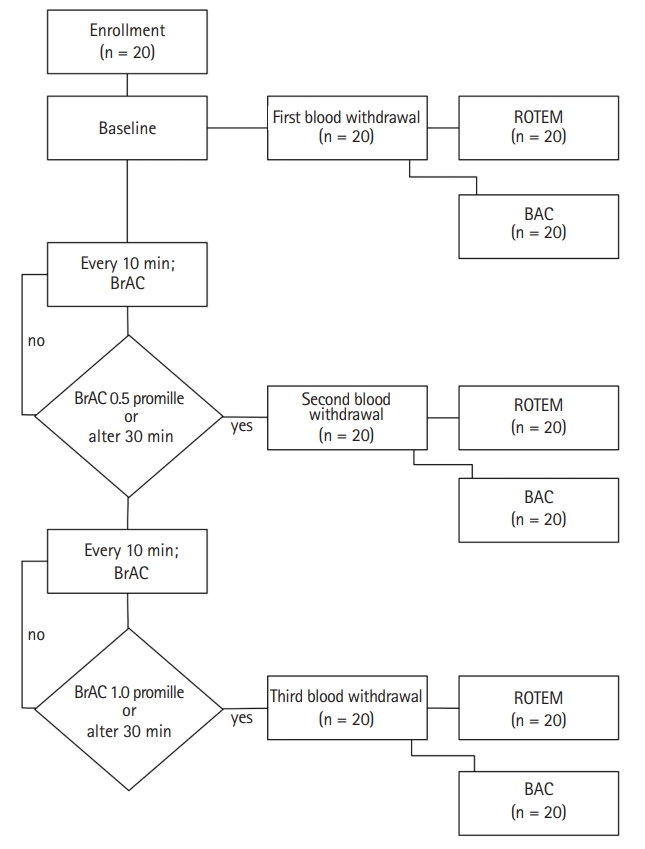
All volunteer participants were employees of the ŌĆ£Department of Anaesthesiology and Intensive Care MedicineŌĆØ at Hannover Medical School who provided informed consent at least one day before our study. The participants were physically and mentally healthy at the time of the study and had consumed no alcohol for seven days and reported no other oral ingestion for a minimum of six hours before the study. Furthermore, the participants had no intake of any long-term or any other kind of medication for seven days. The study took place at the departmentŌĆÖs Christmas party. Our point-of-care setup is shown in Fig. 1. The study outline is depicted in Fig. 2.
Calculated alcohol intake
The target blood alcohol concentration was 1ŌĆ░. Individually required alcohol amounts were calculated according to the Widmark formula [22]. For a study period of one hour, we calculated alcohol depletion in g as "1 hour ├Ś body weight in kg / 10." The formulas "alcohol in g = (body weight in kg ├Ś 0.6 ├Ś 1.0ŌĆ░) ŌĆō 1 hour ├Ś body weight in kg / 10" and "alcohol in g = (body weight in kg ├Ś 0.7 ├Ś 1.0ŌĆ░) - 1 hour ├Ś body weight in kg / 10" were used for female or male volunteers, respectively.
The participants were requested to drink the calculated amounts of alcohol within one hour. Alcoholic drinks (whisk[e]y, vodka, red wine) were selected according to individual preferences; the amounts were adjusted to the respective ethanol concentrations.
Blood sampling
Three blood samples were taken from a cubital vein. Butterfly cannulas (Safety-Multifly-Set®, Sarstedt, Inc., Germany) and several test tubes (S-Monovette® and Citrat-Monovette®, Sarstedt, Inc., Germany) were used. The first milliliter of blood drawn was discarded before each sampling.
The first sample was taken as a baseline measurement before ethanol ingestion. The second sampling was conducted when the breath alcohol concentration was approximately 0.5ŌĆ░. The third blood collection was performed when the breath alcohol concentration was approximately 1.0ŌĆ░ but not more than one hour after the initial alcohol ingestion. We assumed a maximum blood alcohol concentration one hour after ingestion with no further increase in blood alcohol concentration over time. The findings reported by Mitchell et al. [23] support our assumption. Each volunteer served as his/her own control.
Breath alcohol concentration (BrAC)
BrAC was measured in this study with an AlcoMed 3011 breath alcohol testing device (Envitec-Wismar GmbH, Germany). The device was calibrated and serviced 14 days before the study by authorized personnel. For measurement, the volunteer blew into the device with sufficient pressure, evenly and without interruption, until the device sounded a continuous tone. The result was presented in ŌĆ░ BrAC.
Samples were taken after the volunteer had abstained from smoking for at least five minutes and rinsed his/her mouth with water. The volunteers were instructed to breathe normally for at least two minutes before sampling. The mouthpieces were replaced for each measurement.
ROTEM
ROTEM (TEM International GmbH, Munich, Germany) (we used the ROTEM delta system) is a viscoelastic coagulation-testing device that has been described elsewhere in detail [24]. The "ExTem" and "FibTem" ROTEM measurements were initiated without delay after blood withdrawals.
Blood alcohol concentration (BAC)
The Department of Forensic Medicine at the Hannover Medical School measured the BAC.
Headspace gas chromatography was used for serum ethanol concentration analysis. Chromatographic separation was performed on a CBK-B 60/80, 1 m ├Ś 2.0 mm (Restek GmbH, Germany) column on a Clarus 480 gas chromatograph and a Turbo matrix 110 headspace sampler (Perkin Elmer, Inc., USA).
Testing for the presence and subsequent quantification of ethanol in blood was carried out in static headspace mode. All samples were prepared and injected in duplicate. Linear regression analysis was used to generate calibration curves with duplicate measurements of aqueous calibration standards (0.5, 1.0, 2.0, 3.0, 4.0, and 5.0 mg/L). The limit of quantification was 0.1 mg/L. The intra-day precision (expressed as percent relative standard deviation [%RSD]) and the accuracy (expressed as % bias) of the method were 5% and 7%, respectively. Serum ethanol concentrations were converted into BAC as usual for forensic blood ethanol analysis [25,26].
Statistics
Demographic data included age, sex, weight, and height. The event data were the drinking start and end times, drink amounts and types, and BACs. Ethanol intake was calculated from the ingested beverages as described above.
Data were exported to IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., USA) for further descriptive and explorative data analysis. We applied Wilcoxon tests to compare ROTEM data. P values < 0.05 were considered statistically significant. For multiple comparisons, P values were calculated using the HolmŌĆōBonferroni method.
Results
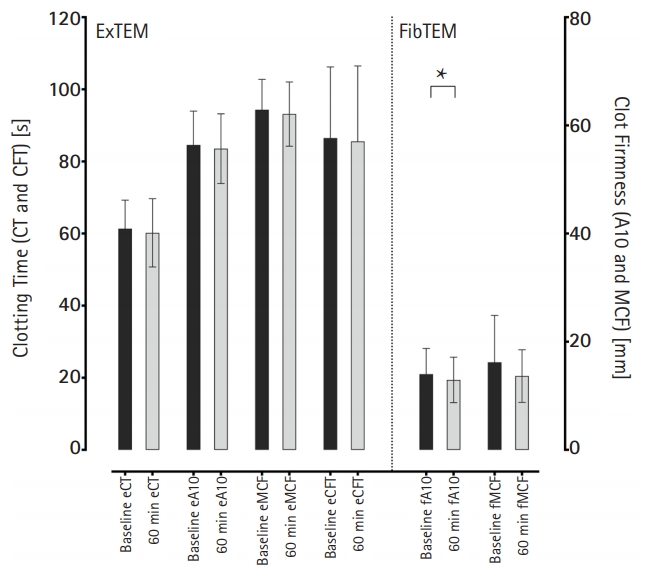
We examined a total of 20 healthy volunteers comprising eleven men (55%) and nine women (45%). Their mean age was 29.4 ┬▒ 6.0 years and their mean height and weight were 177.5 ┬▒ 8.6 cm and 77.7 ┬▒ 16.5 kg, respectively. The resulting mean body mass index (BMI) was 24.6 ┬▒ 4.2 kg/m┬▓. The basic participant data are summarized in Table 1. Each participant could choose between three types of alcohol: 10% chose red wine, 30% chose whisk(e)y, and 60% chose vodka. The volunteers consumed a mean of 51.29 ┬▒ 13.51 g ethanol each. The first blood withdrawal before ethanol consumption showed a BAC of 0.00 ┬▒ 0.0ŌĆ░ for all participants. The mean BACs were 0.48 ┬▒ 0.3ŌĆ░ and 0.76 ┬▒ 0.2ŌĆ░ for the second and third blood samples, respectively. The detailed results of our ROTEM (ExTEM and FibTEM) analysis of the blood samples are shown in Table 2. We focused on the ExTEM and FibTEM clotting time (eCT), clot amplitudes after ten minutes (eA10/fA10), maximum clot firmness (eMCF/fMCF), and maximum lysis (eML/fML). The mean eCT baseline value was 61.4 ┬▒ 7.9 s. At the one-hour blood collection, the eCT was 60.2 ┬▒ 9.5 s. The A10 value indicates the amplitude of the ROTEM trace 10 minutes after the start of clotting. The eA10 and fA10 values were 56.4 ┬▒ 6.2 and 14.0 ┬▒ 4.8 mm, respectively. After consumption of the whole volume of ethanol, the eA10 and fA10 values were 55.7 ┬▒ 6.5 and 13.0 ┬▒ 4.2 mm, respectively. The mean eMCF was 62.9 ┬▒ 5.6 mm in the first blood sample and 62.1 ┬▒ 6.0 mm in the last sample. Regarding FibTEM, the fMCF was 16.2 ┬▒ 8.7 mm at baseline and 13.7 ┬▒ 4.9 mm at one hour. We saw no hyperfibrinolysis in the 60 ROTEM measurements, which we assumed to indicate a maximum lysis (ML) > 15%. Furthermore, we saw no significant difference in any fibrinolysis parameter. Comparisons of ROTEM parameters revealed no significant differences.
Sex aspects
Our study included 9 female and 11 male participants. Our subgroup analysis divided by sex showed no significant differences in the measured ROTEM parameters in the female subgroup (Table 3). The male subgroup showed a significant difference in fA10 FibTEM value (P = 0.042, Table 3 and Fig. 3). We observed no significant differences in age, height, weight, and BMI. The female volunteers had to drink significantly less ethanol to reach the 1ŌĆ░ target (P = 0.001) and had a significantly lower mean BAC than that in the male participants after the one-hour period (0.62 ┬▒ 0.2ŌĆ░ vs. 0.87 ┬▒ 0.2ŌĆ░, P = 0.004).
Discussion
This study determined the in-vivo effect of alcohol consumption on coagulation measured by ROTEM. In our healthy participants, we observed a significant change in the fA10 value for early fibrin-clot (FibTEM). The other parameters were not significantly influenced by alcohol intake.
The reduced fA10 amplitude combined with a lower fMCF suggested that a moderate level of about 0.8ŌĆ░ blood alcohol can affect fibrinogen polymerization. This finding is in line with the results of previous studies reporting fibrinolysis impairment [11-13], reduced fibrin formation and fibrin cross-linking rates [3], and reduced fibrinogen and fibrin functionality [10,13]. In a ROTEM-based study of more than 400 trauma patients, Howard et al. [27] showed a bidirectional effect on coagulation related to ethanol ingestion. They demonstrated an initially impaired clot formation and a subsequent inhibition of fibrinolysis. They assumed these balancing mechanisms made a supposed correlation of altered ROTEM measurements and outcome in ethanol intoxicated trauma patients very difficult. However, we did not observe impaired fibrinolysis in our healthy volunteers. The underlying mechanisms appear to be specific to the condition of severe trauma in combination with ethanol ingestion.
We observed a significant difference in the fA10 value in our male subgroup but not in the female subgroup. Spoerke et. al. [3] reported that sex was an independent factor impacting the coagulation system and the influence of ethanol on hemostasis. They found a significantly decreased clot formation speed and reduced cross-linking of fibrin after alcohol ingestion in healthy male volunteers. Generally, the outcome after severe trauma differs between men and women [28,29]. However, in our study, the male participants had significantly higher BAC after one hour than that in the female volunteers.
De Lange et al. [10] reported inhibition of platelet adhesion to fibrinogen after intake of alcohol in alcopops (Barcardi Breezer) but not red wine (Rioja). Thus, the alcohol type can affect coagulation alterations, particularly fibrin polymerization. Unfortunately, in our study, only two participants (10%) chose red wine. Therefore, a comparison of different kinds of alcohol to red wine was not possible.
We were unable to fully reproduce Engstr├ČmŌĆÖs in-vitro results in our in-vivo approach, as they showed strong disturbances of overall clot formation. CFT, which indicates the dynamics of clot formation, was reduced by 34% at an ethanol concentration of 1ŌĆ░, and by 118% at 4ŌĆ░, respectively [11]. Moreover, they observed reduced fibrinolysis. In our study, neither the dynamic parameters nor fibrinolysis differed after alcohol intake. All participants consumed a calculated amount of ethanol to reach a 1ŌĆ░ BAC. For obvious reasons, for the in vivo setting, we did not take the 2 or 4ŌĆ░ conditions into account. With a mean BAC of 0.76ŌĆ░, we did not reach the calculated and targeted 1ŌĆ░ within one hour. Engstr├Čm and colleagues used 96% pure ethanol added directly to a test tube, obviously without any additives. This and different metabolites of ingested ethanol such as acetaldehyde may impair the assays differently [30]; furthermore, we allowed different types of alcohol (red wine, whisk[e]y and vodka). Moreover, we used citrated blood sample tubes. Naturally, Engtr├Čms et al. established no correlation to the in-vivo situation due to the limitations of the in-vitro setting.
Based on our results, the implications for daily clinical practice remain unclear. Although the absolute reduction in fibrin clot firmness was only 1 mm at fA10 and 3 mm at fMCF, in patients with underlying coagulopathy (e.g., trauma patients), additionally impaired coagulation due to alcohol might affect bleeding, clinical outcome, and clinical therapeutic decisions.
Alcohol is a socially accepted and commonly used drug. Moderate amounts are even considered to be protective of the cardiovascular system [31,32]. The impact of acute ethanol intake on coagulation and the parameters of coagulation still require elucidation and are hotly debated. Some studies found no effect, particularly with regard to standard coagulation measurements and hemorrhagic complications [14]. Others described multiple effects of ethanol on the coagulation system such as alterations in platelet function and prolonged bleeding time [9] or inhibition of platelet adhesion to fibrinogen [10]. Point-of-care coagulation assessment by ROTEM or TEG has become a routine option in the last decade as it is considered to be a better predictor of clinical bleeding tendency than other coagulation tests [33,34]. Furthermore, it appears to be more sensitive and specific than routine coagulation tests in detecting impairments of the coagulation system [34-37]. ROTEM/TEG analysis evaluates hemostasis more holistically than the standard coagulation test. These tests allow the detection of whole clot formation, fibrinogen-platelet interactions, and hyperfibrinolysis [24].
A trial investigating hemostasis in 264 trauma patients with elevated ethanol blood concentration reported impaired clot formation in TEG assays; however, the elevated blood concentration was not predictive for transfusion requirements or early or late mortality. The authors concluded that ethanol potentially directly affected the TEG measurements and that further studies were needed [38].
Nevertheless, a significant number of patients in the emergency department are under the influence of higher BACs [2ŌĆō5]. Trauma mortality increases with blood ethanol level [19,20] and trauma combined with ethanol is associated with increased blood loss requiring volume resuscitation and red blood cell transfusion [21]. Massive hemorrhage is one of the leading causes of death in trauma patients, accounting for approximately 40% of trauma deaths [39]. Furthermore, the trauma itself can cause a hemostasis imbalance known as TIC [40], which may lead to increased bleeding if alcohol intoxication is an additional factor. TIC is a complex mechanism triggered by hypoperfusion and activated protein C that eventually leads to hypofibrinogenemia, hyperfibrinolysis, impaired fibrinogen polymerization, and subsequent inhibition of normal clot formation, especially in cases of extensive tissue trauma [41,42]. Extrapolating our results, it could be presumed that alcohol might aggravate hemostasis impairment. One conceivable mechanism besides the direct impairment of fibrinogen polymerization is that alcohol-positive trauma patients had elevated base excess levels compared to trauma patients without alcohol with comparable severities of injury [38]. Hess et al. [1] described the coagulopathy of trauma as a situation in which acidemia itself impairs plasma protease function and coagulation factor complex activity. Ethanol or its metabolites may aggravate acidemia and, therefore, contribute to the alteration of coagulation.
This study has several limitations: we did not reach the average blood alcohol target of 1ŌĆ░ in every volunteer, which limits the comparability of our data. Moreover, the type of alcohol was freely selectable. Because of this, the discrimination of specific type-dependent alcohol effects was complicated. Furthermore, the sample size was not powered to show specific sex effects. In addition, all participants were healthy.
In conclusion, our results showed a moderate impairment of thrombelastometric measurements, limited to early fibrin clot formation, in healthy volunteers. However, the fibrin-clot, determined by thrombelastometric methods, is expected to diminish after usual alcohol intake with the potential risk of falling below critical levels if other coagulation impairments supervene. Further studies are needed to evaluate the influence of ethanol itself on thromboelastometry and to determine the effects of acute ethanol intoxication on hemostasis, particularly in trauma patients.